Session Information
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: Conventional Disease Activity Score 28 has variable sensitivity, subjectivity, inherent bias due to certain variables such as more weightage to joint tenderness and overestimation due to pain component. Ultrasound is a more sensitive, objective, reproducible and an overall better tool for detection of synovitis. We compared a composite ultrasound-based index ECODAS (echographic disease activity score) with DAS28 in patients with rheumatoid arthritis (RA).
Methods: This was a cross-sectional study involving patients with RA (according to ACR criteria) attending OPD in a tertiary care institution. DAS28 score was calculated using tender joint count (TJC), swollen joint count (SJC), ESR, CRP and patient’s response. Ultrasound scan of same 28 joints was performed by a single observer, blinded to clinical information, using latest US device with a high frequency (8-13 MHz) linear transducer – longitudinal and transverse scan of shoulders (posterior recess for glenohumeral joint, anterior recess for bursitis and bicipital tendon sheath), elbows (anterior, lateral and posterior recess), wrist (radioulnar, radiocarpal and intercarpal), hands (dorsal and volar aspect of 1-5 metacarpophalangeal joint and 1-5 proximal interphalangeal joint) and knees (supra patellar and para patellar recesses). We evaluated the number of joints with synovitis in gray scale (NGSUSJ) and the number of joints with Doppler signal (NPDUSJ). A composite ultrasound-based index was calculated using formula of DAS28 score, substituting clinical variables with sonographic variables i.e. ECODAS1- NGSUSJ in place of NTJ and PDUSJ in place of NSJ, and vice versa for ECODAS2.
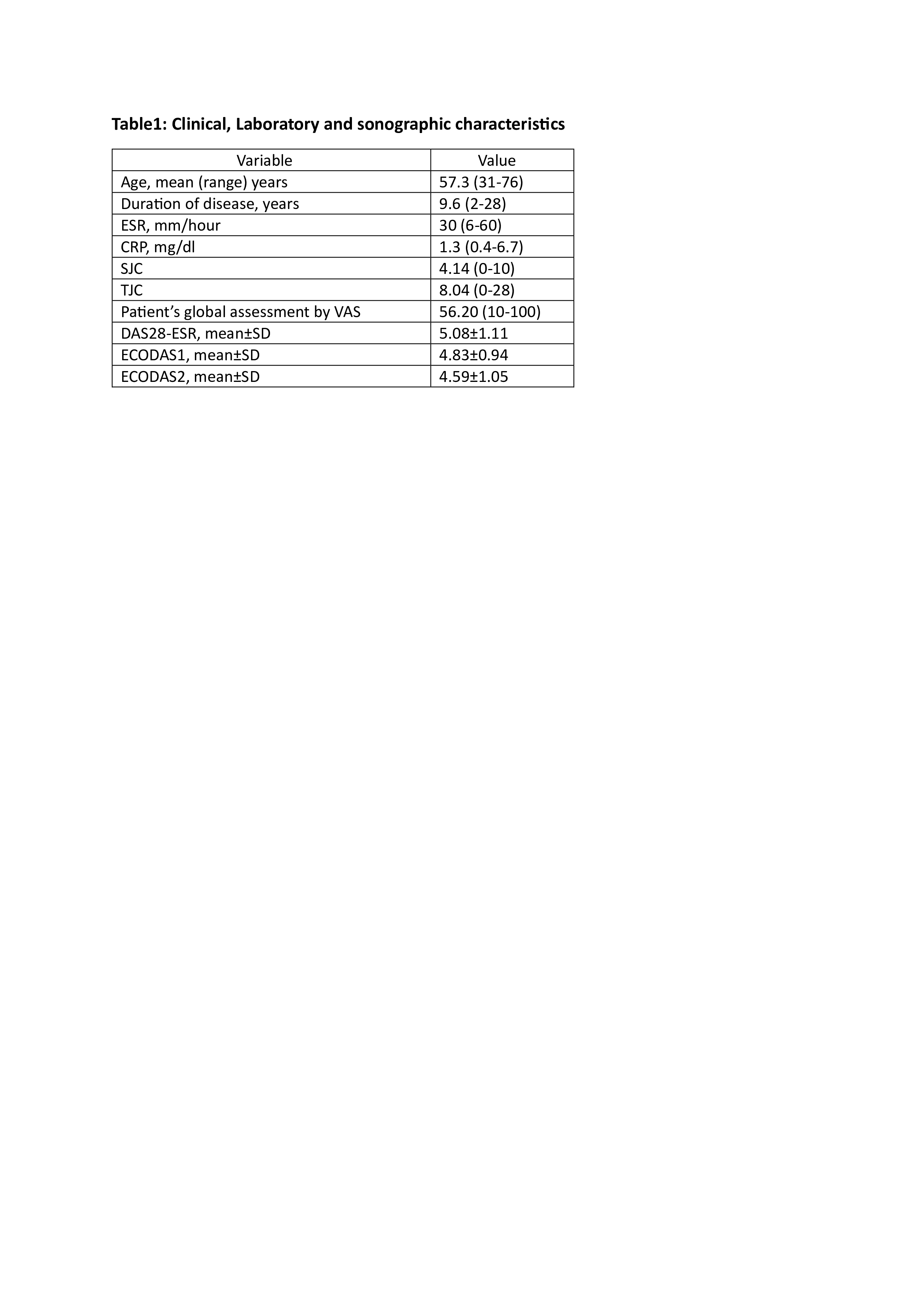
Results: We included 76 patients (78.94% women), 71 patients were receiving DMARDs and 5 were on combined DMARDs and biological therapy. The clinical, lab and US variables are presented in Table1. Good agreement was observed between swollen joints and synovitis by GSUS and PDUS. The average agreement between TJ and GSUS was 71% and between SJ and PDUS was 86%. The clinical and ultrasonographic index demonstrated statistically significant correlation with Pearson coefficient of 0.61 (p < 0.00001) between ECODAS1 and DAS28 and of 0.54 (p < 0.00001) between ECODAS2 and DAS28. However significant difference (Pearson’s coefficient of 0.16) was observed between the two indices (ECODAS1 < DAS28) at higher range of DAS28 scores (DAS28 > 5.1) with high TJ counts, due to influence of pain component.
Conclusion: ECODAS has shown good correlation with DAS28 in most cases except the subset with high disease activity. US evaluation of inflammatory joints in RA with ECODAS1 is an objective method of assessment of disease activity, which can eliminate the bias due to pain in DAS28. Hence a combination of clinical, laboratory and ultrasonographic parameters can prove a better assessment tool of disease activity.
To cite this abstract in AMA style:
Verma Saluja K, Khokhar H, Sharma A, Chittora S. Assessment of Correlation Between Composite Ultrasonographic Index (ECODAS) and Disease Activity Score 28 in Patients with Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/assessment-of-correlation-between-composite-ultrasonographic-index-ecodas-and-disease-activity-score-28-in-patients-with-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/assessment-of-correlation-between-composite-ultrasonographic-index-ecodas-and-disease-activity-score-28-in-patients-with-rheumatoid-arthritis/