Session Information
Session Type: Abstract Session
Session Time: 10:45AM-11:00AM
Background/Purpose: Axial gout involvement was first reported in 1950 (1). Over 100 cases have subsequently been published. Reported cases have presented as acute back pain, cord compression, and/or neurologic symptoms, with diagnosis made by invasive procedure (surgical excision or biopsy). However, the true extent of MSU deposition in the spine of gout patients, including asymptomatic patients or those with non-specific symptoms, is unknown and likely higher. We used DECT to determine the extent of MSU deposition in the lumbosacral spines of patients with gout, with and without tophi, compared to controls without gout.
Methods: We recruited controls, nontophaceous, and tophaceous gout patients, age 45-80. Individuals with CPPD disease, RA, spondyloarthropathy, active spinal malignancy, or on urate lowering treatment (ULT) ≥ 6 months were excluded. Gout subjects met 2015 ACR gout classification criteria, with entry serum urate (sU) of >6.8 mg/dL ( >6.0 mg/dL if on ULT for < 6 months). Demographics, gout history, Aberdeen back pain scale, sU, ESR, and CRP were collected. Subjects underwent DECT of the lumbosacral spine (LS) to assess for MSU deposition.
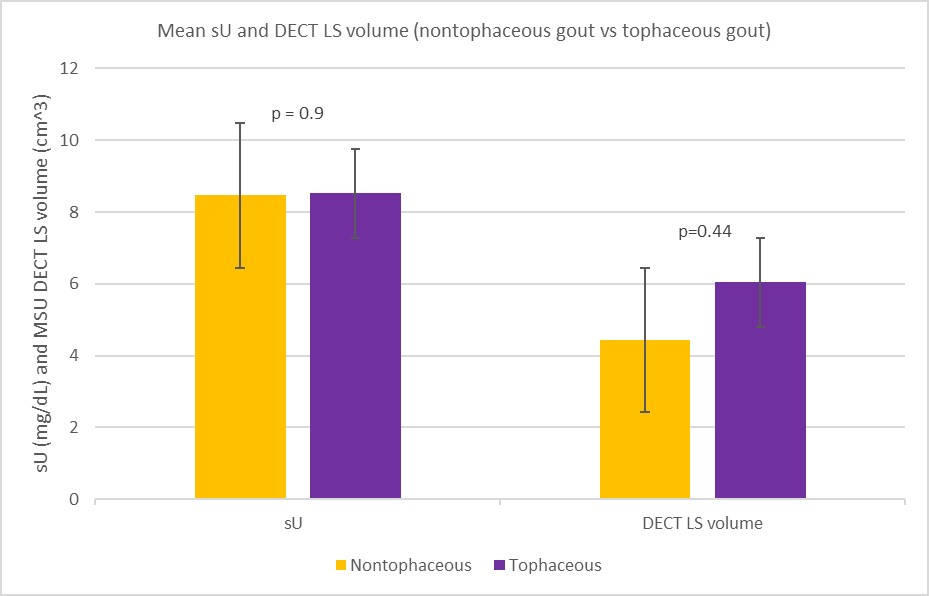
Results: 75 subjects were enrolled, and 72 completed the study (1 nontophaceous gout patient lost to follow-up prior to DECT, 2 tophaceous excluded after sU at time of DECT found to be < 6.0mg/dL). All groups were similar in age in years (controls 61.8±3.8, nontophaceous 64.0±6.1, tophaceous 60.4±11.0, p=0.81) but differed in BMI (controls 28.3±6.5 kg/m2, nontophaceous 34.1±7.2 kg/m2, tophaceous 29.5±4.5 kg/m2, p=0.03) and creatinine (controls 1.0±0.2 mg/dL, nontophaceous 1.4±0.7 mg/dL, tophaceous 1.4±0.6 mg/dL, p< 0.05). Mean sU and ESR were higher in gout subjects (sU-controls 5.3±1 mg/dL, nontophaceous 8.5±1.7 mg/dL, tophaceous 8.5±1.6 mg/dL, p< 0.05; ESR-controls 13.7±13.8 mm/h, nontophaceous 26.5±19.4 mm/h, tophaceous 25.1±15.7 mm/h, p< 0.05). Using standard DECT settings for MSU visualization, gout patients had larger MSU volumes than controls (controls 2.2±1.2 cm3, all gout 5.23±6.9 cm3; p =0.03). Tophaceous patients had numerically greater MSU deposition compared with nontophaceous (6.0±8.9 cm3, vs 4.4±4.3 cm3, ns). Reanalysis of a subset of scans using highly specific settings to eliminate artifact reduced the number of subjects with MSU signal but confirmed greater prevalence of deposition among gout patients (n=29; controls with deposition 0/9, nontophaceous with deposition 1/11, tophaceous with deposition 2/9). Back pain was also more common among gout patients. No subject had frank tophi on spinal DECT.
Conclusion: Gout patients have significantly greater intercritical inflammation and LS MSU deposition than controls, and trend toward greater deposition among patients with tophi. Preliminary results using the most stringent DECT threshold settings suggests MSU differences are not artifact. The complete data set is currently undergoing evaluation and the full results will be presented.
Supported by an investigator-initiated grant from Horizon Pharma.
References:
1. Toprover M, Krasnokutsky S, Pillinger MH. Gout in the Spine: Imaging, Diagnosis, and Outcomes. Curr Rheumatol Rep. 2015;17(12):70.


To cite this abstract in AMA style:
Toprover M, Mechlin M, Slobodnick A, Pike V, Oh C, Davis C, Fields T, Becce F, Pillinger M. Assessing the Extent of Lumbosacral Spinal Urate Deposition in Patients with Tophaceous and Nontophaceous Gout Compared with Non-gout Controls Using Dual-Energy CT (DECT) [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/assessing-the-extent-of-lumbosacral-spinal-urate-deposition-in-patients-with-tophaceous-and-nontophaceous-gout-compared-with-non-gout-controls-using-dual-energy-ct-dect/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/assessing-the-extent-of-lumbosacral-spinal-urate-deposition-in-patients-with-tophaceous-and-nontophaceous-gout-compared-with-non-gout-controls-using-dual-energy-ct-dect/