Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Achievement of a lupus low disease activity state (LLDAS) has been associated with less organ damage, fewer disease flares, and improved health-related quality of life in children with systemic lupus erythematosus (cSLE). A consensus-based definition for childhood lupus low disease activity state (cLLDAS) was recently proposed by the international childhood lupus T2T task force. Our objective was to determine the baseline frequency of data collection necessary to calculate cLLDAS across multiple pediatric rheumatology clinics.
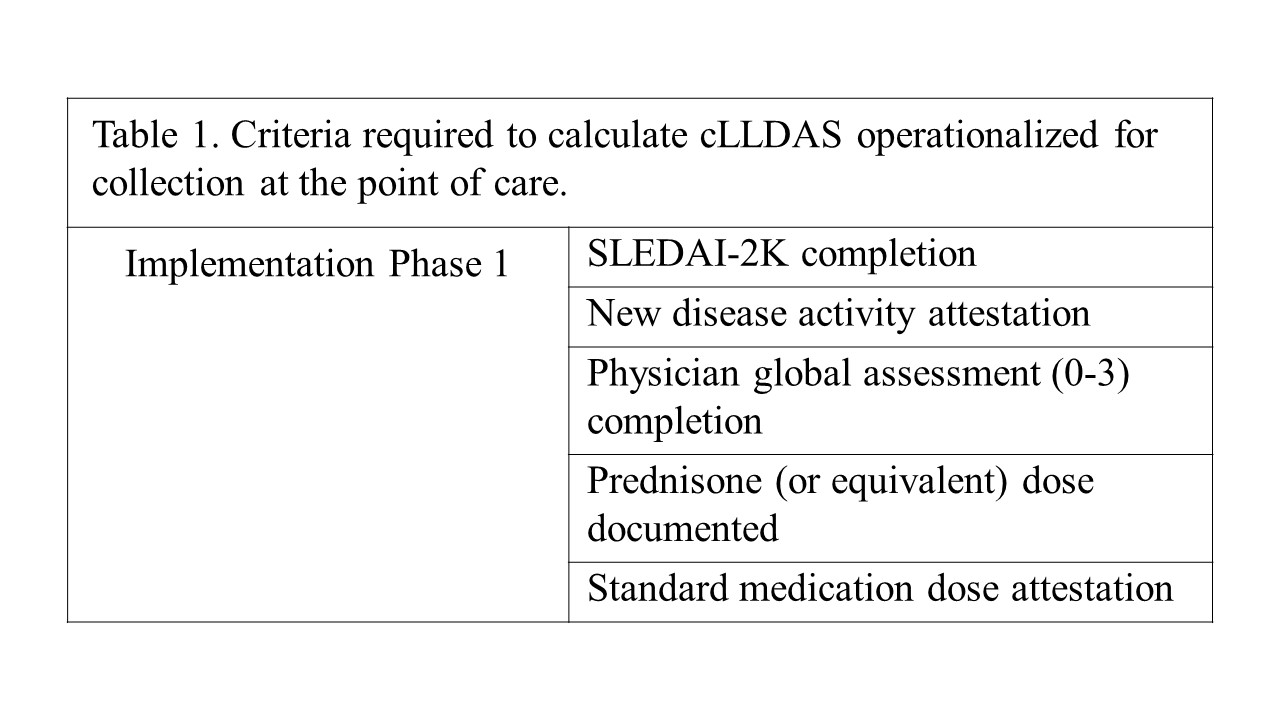
Methods: The Pediatric Lupus Understanding Systems (PLUS) collaborative was formed consisting of 5 pediatric rheumatology sites located in children’s hospitals affiliated with academic medical centers in the United States. We operationalized the 5 cLLDAS criteria to collect at the point of care (Table 1) and updated data fields within the electronic health record (EHR) at each site as needed to facilitate structured data collection. Eligible visits were defined as ambulatory visits in the pediatric rheumatology clinic with an SLE diagnosis code (ICD-10-CM M32.* excluding M32.0). We collected the percentage of eligible visits across all sites each month in which data was collected for each cLLDAS criteria. We then plotted performance over time on statistical process control charts.
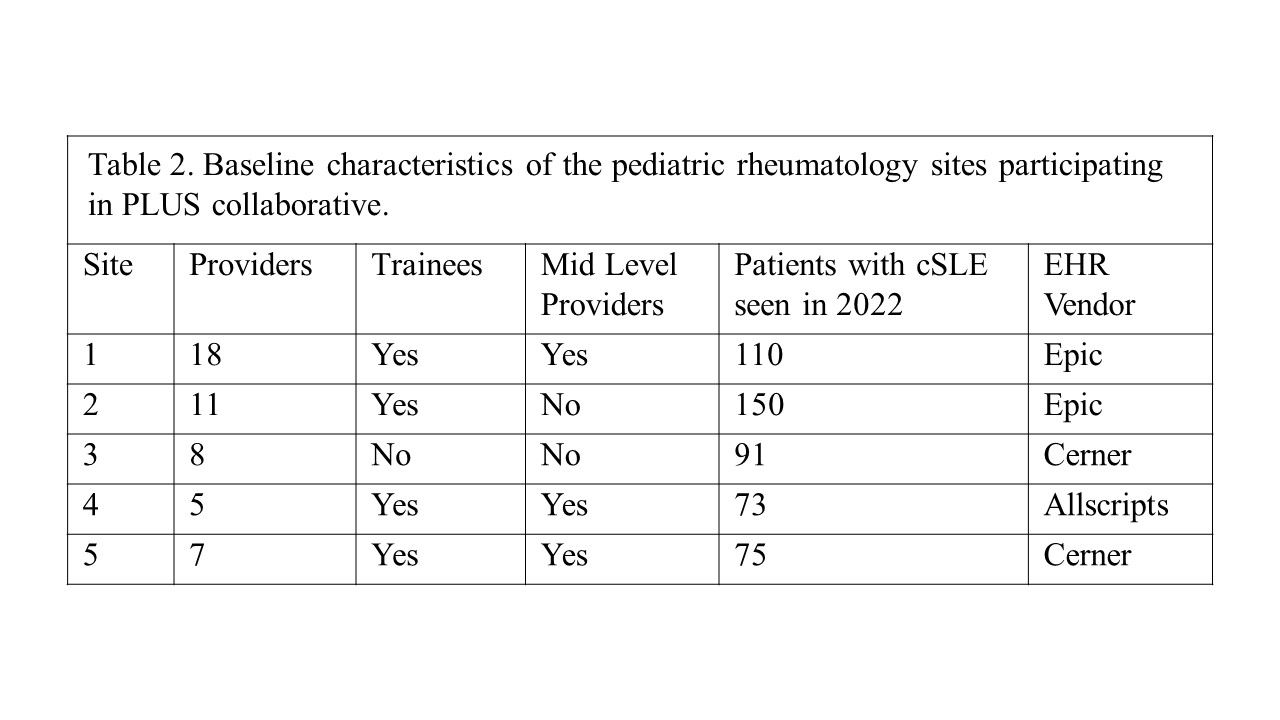
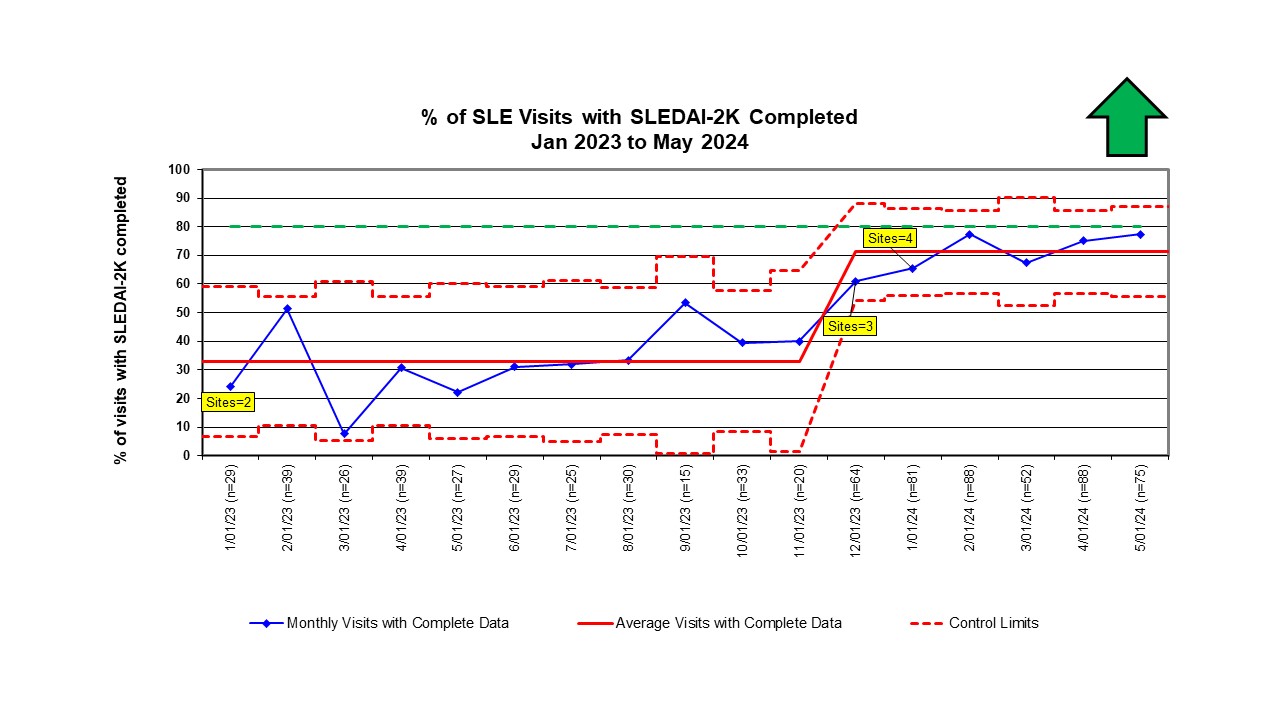
Results: We collected a baseline implementation assessment from each PLUS collaborative site leader (n=5). Sites reported a range of number of pediatric rheumatology providers (5-18), most had trainees in clinic, and 3 sites include mid-level providers (Table 2). The approximate number of patients with cSLE seen in 2022 varied from 73-150 with a broad mix of insurance. All major EHR vendors are represented. From January 2023 through May 2024, we analyzed data from a total of 760 visits for patients with cSLE across 4 sites. SLEDAI-2K was completed at an average of 33% of visits at baseline with improvement to 71% once additional sites were added (Figure 1). “No new disease activity” attestation was not collected until December 2023 with completion in 33% of visits through May 2024. A physician global assessment of 0-3 was completed in 14% of visits, but a physician global assessment of 0-10 was completed in 51% of visits. Prednisone or equivalent dose was recorded in 39% of visits, and other immunosuppressant medications were documented in 38% of visits starting in December 2023.
Conclusion: Baseline collection of the data elements necessary to calculate cLLDAS at lupus visits across multiple well-resourced pediatric rheumatology sites is unreliable. Additional interventions are needed to improve data collection to facilitate cLLDAS assessment at the point of care. A structured implementation program will be required to implement a treat to target approach to decision making for childhood lupus in real-world clinical practice.
To cite this abstract in AMA style:
Smitherman E, Harris J, Hersh A, Huggins J, Lytch A, Ho H, Meyer A, Quinlan-Waters M, Timmerman L, Burnham J. Assessing Lupus Low Disease Activity State in the Pediatric Rheumatology Clinic: Baseline Data Collection from a Pediatric Lupus Collaborative [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/assessing-lupus-low-disease-activity-state-in-the-pediatric-rheumatology-clinic-baseline-data-collection-from-a-pediatric-lupus-collaborative/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/assessing-lupus-low-disease-activity-state-in-the-pediatric-rheumatology-clinic-baseline-data-collection-from-a-pediatric-lupus-collaborative/