Session Information
Date: Saturday, November 6, 2021
Title: SLE – Diagnosis, Manifestations, & Outcomes Poster I: Diagnosis (0323–0356)
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: The APOL1 gene is implicated in induction of TLR3 agonists and interferons as well as in autophagy. Two genetic variants, G1 (2 single nucleotide polymorphisms) and G2 (6 base pair deletion) have been selected evolutionarily as protective against Trypanosoma. These APOL1 high risk allelles are associated with progression to end stage renal disease (ESRD), including lupus nephritis, and in one study with avascular necrosis in SLE. We examined the association of APOL1 in ESRD, avascular necrosis, atherosclerotic events and pulmonary fibrosis in African-American SLE.
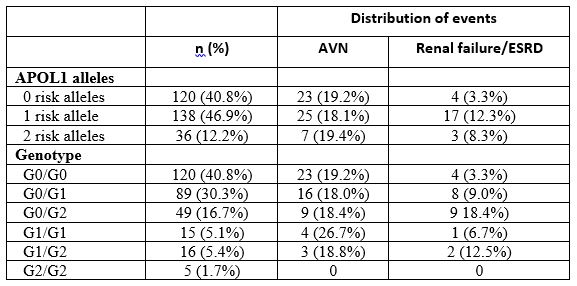
Methods: APOL1 G1 (rs73885319 and rs60910145) and G2 (rs71785313) genetic variants were genotyped in 294 SLE African American patients in the Hopkins Cohort using TaqMan assays (Thermofisher Scientific, Waltham MA ). APOL1 variants were classified as G1/G1 homozygous (in our dataset, G/G), G2/G2 homozygous (-/-), compound heterozygous G1/G2 (G/T or A/G AND TTATAA/-), G0/G1 heterozygous (G/T or A/G), or G0/G2 heterozygous (TTATAA/-). Based on the variants, patients were stratified into groups with 0, 1, or 2 risk alleles. To address the association between APOL1 group and the three outcomes, we used Kaplan Meier approach to estimate the distribution of time to outcomes from date of birth and log-rank test to compute the p-value. Cox regression was used to estimate the hazard ratio and adjust the relationships. The follow up for each patient ended at the patient’s last cohort visit, or at the time of their first event.
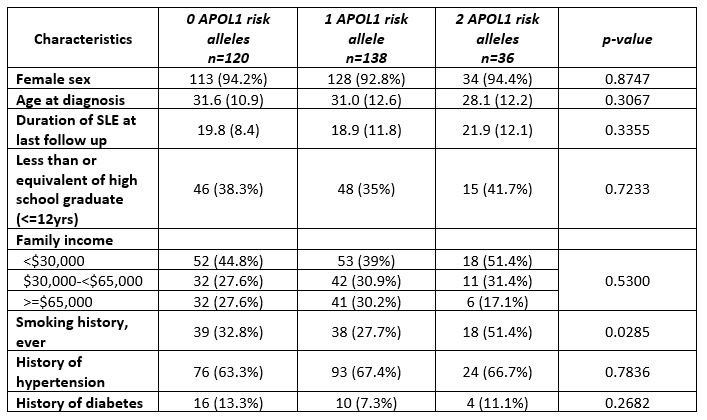
Results: 294 African American patients were included in the analysis. 275 (93.5%) were female. The frequency of two copies of the APOL1 risk allele was 12.2% (Table 1). There was a higher proportion of patients with smoking history in the group with 2 risk alleles compared to the low risk groups (Table 2). There was an association with ESRD, but not with AVN, pulmonary fibrosis or cardiovascular events (Table 3).
Conclusion: Our study showed a significantly higher risk of progression to renal failure/ESRD among those with at least one risk allele, with a hazard ratio of 3.50 (p=0.0234 after adjusting for sex, ever smoking and hypertension). We did not find an association between APOL1 risk alleles and avascular necrosis/ atherosclerotic events/pulmonary fibrosis. Our analysis included adjustment for smoking, as it is a risk factor for all the outcomes, and included larger numbers of African-American patients and outcomes than previous studies.

To cite this abstract in AMA style:
Petri M, Kallas R, Li J, Magder L, Goldman D. Apolipoprotein L1 (APOL1) in African-American SLE: Frequency and Clinical Associations [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/apolipoprotein-l1-apol1-in-african-american-sle-frequency-and-clinical-associations/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/apolipoprotein-l1-apol1-in-african-american-sle-frequency-and-clinical-associations/