Session Information
Date: Monday, November 13, 2023
Title: Abstracts: Vasculitis – Non-ANCA-Associated & Related Disorders I: Imaging
Session Type: Abstract Session
Session Time: 2:00PM-3:30PM
Background/Purpose: Aortic dilatation is typically a late complication of giant cell arteritis (GCA) but there are no tools to risk stratify patients at the time of diagnosis. We assessed the prevalence of aortic dilatation at 5 years in an inception giant cell arteritis cohort and assessed the relationship with FDG-PET/CT detected vascular activity at diagnosis, 6 months and 5 years.
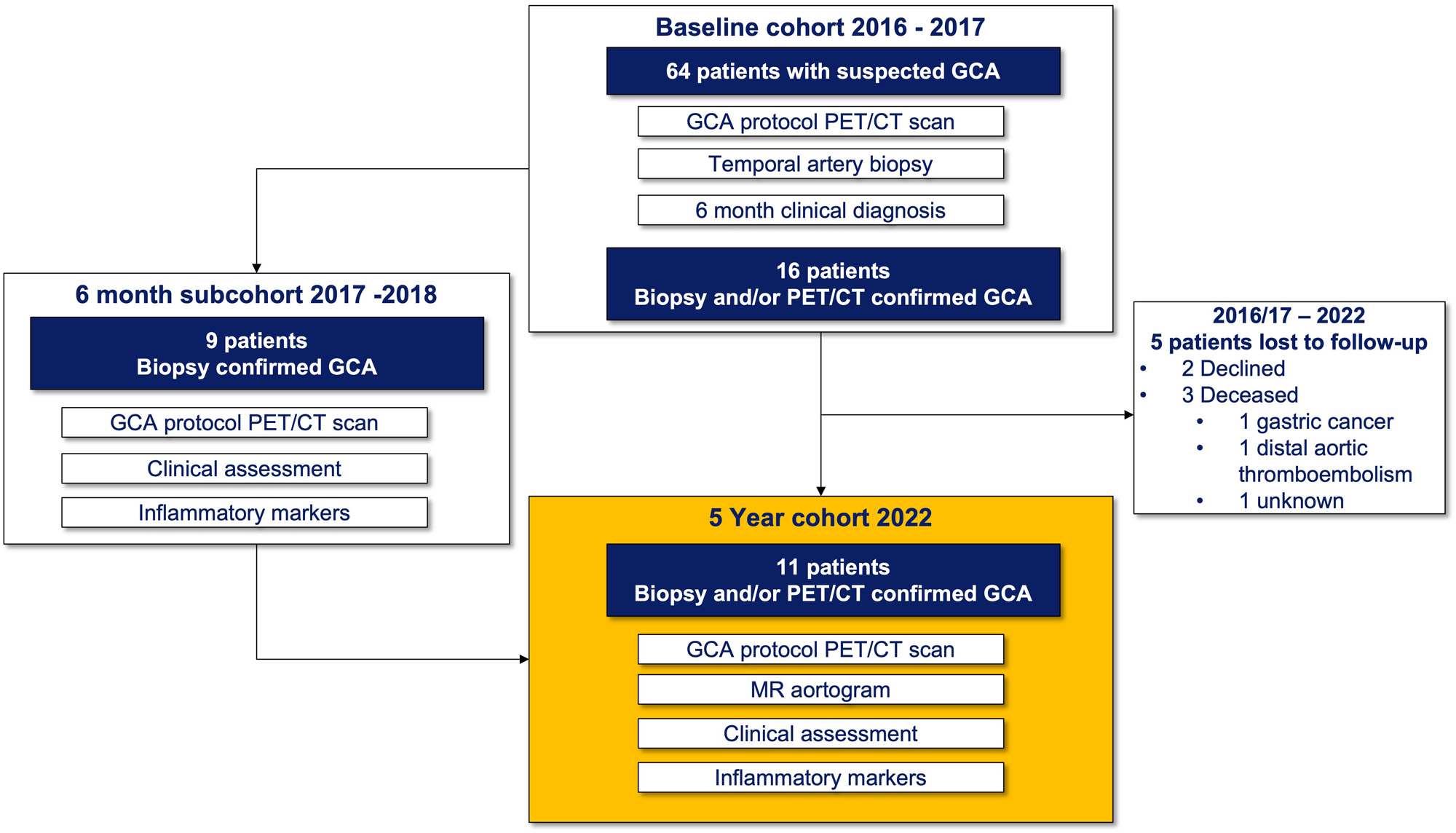
Methods: Patients were eligible for this 5-year study if they had been enrolled in the Giant Cell Arteritis and PET Scan (GAPS) cohort in 2016 or 2017, had a clinical diagnosis of GCA and a positive temporal artery biopsy (TAB) and/or a positive FDG-PET/CT scan at diagnosis. Patients underwent an FDG-PET/CT scan including assessment of cranial and large vessels, non-contrast MRI of the aorta, trans-thoracic echocardiogram (TTE) of the ascending aorta, blood collection and clinical assessment. PET/CT scans were dual reported by 2 blinded nuclear medicine physicians. Scans were reported overall positive or negative for disease activity and a visual grading of FDG avidity in each vascular territory was made with comparison to blood pool. MRI was reported by a single blinded cardiovascular radiologist and thoracic aortic dilatation was defined as external diameter >= 40 mm in ascending or >= 30 mm in the descending aorta.
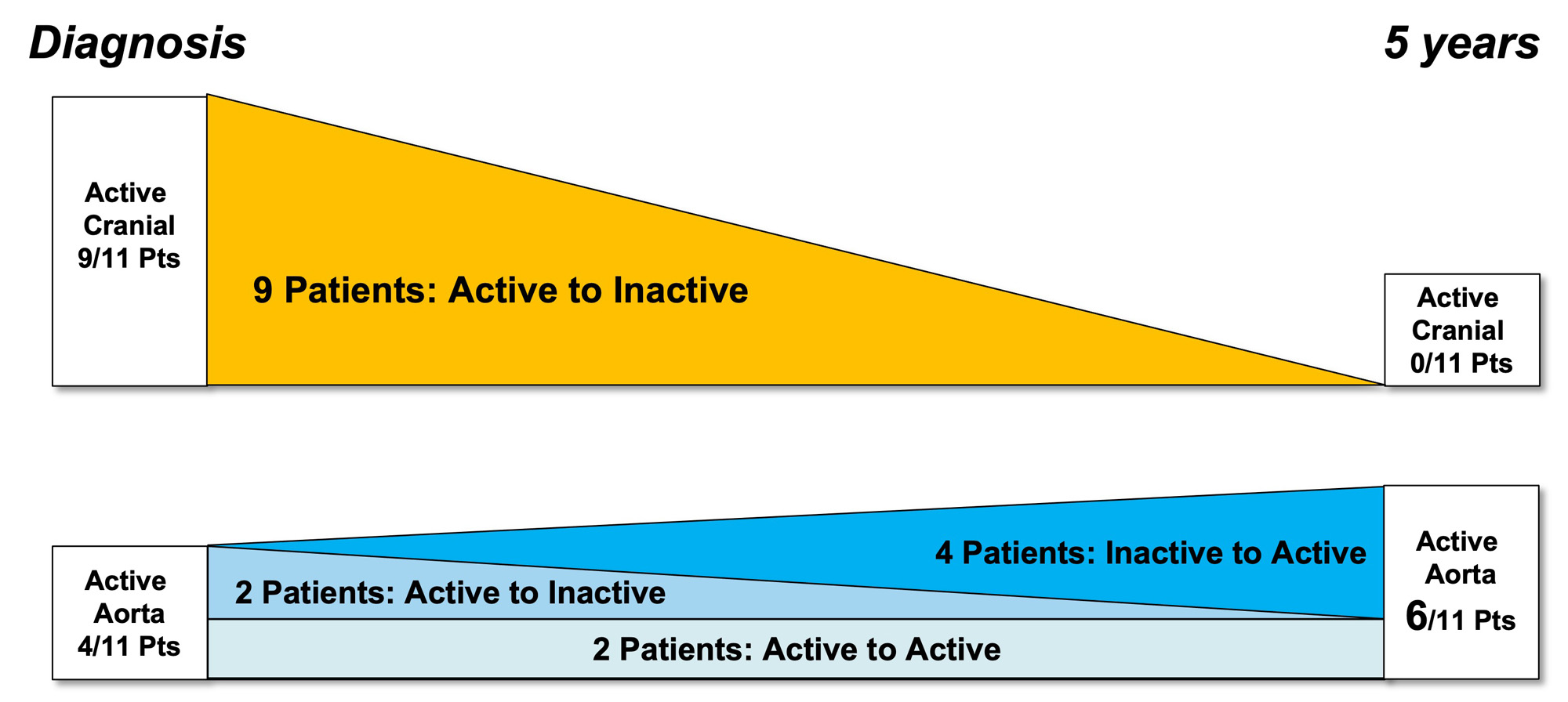
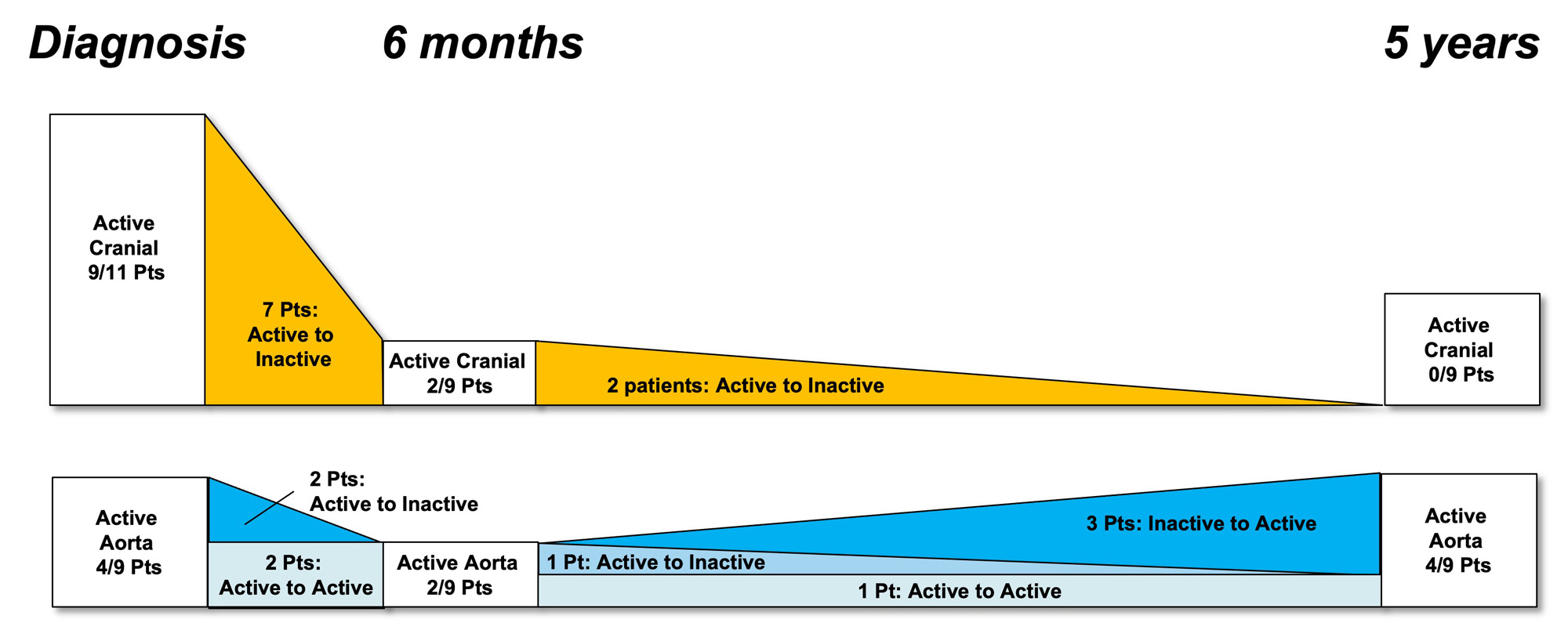
Results: 16 of the original 64 “suspected GCA” patients in the GAPS cohort met inclusion criteria and 11 participated in the 5-year study (3/16 deceased, 2/16 declined). The median age was 75, 73% were female and all were in clinical and serological remission with a median CRP of 1 (range 1 – 8). 4/11 (36%) patients had aortic dilatation (range 40 – 43mm) and 5/11 (45%) had globally active FDG-PET/CT scans. There was a trend towards a higher median aortic diameter in those with positive scans at 5 years (42 mm vs 35 mm, p=0.08) but aortic avidity at diagnosis did not predict 5-year dilatation. The distribution of FDG-PET/CT detected activity changed from a mix of cranial and large vessel disease at diagnosis to exclusively large vessel disease at 5-years. Aortitis developed in 4 patients who previously had inactive aortas. All 6 patients with inactive scans were taking an immunosuppressive agent (methotrexate, leflunomide, azathioprine or tocilizumab) at 5 years while all patients with active scans were not on therapy (p=0.02). TTE had excellent correlation with MRI for maximum aortic diameter (Pearson’s correlation coefficient 0.91).
Conclusion: Aortic dilatation was present in 36% GCA patients at 5 years. The distribution of FDG PET-CT detected avidity changed from predominantly cranial to exclusively large vessel disease and this may explain the lack of association between aortic avidity at diagnosis and dilatation at 5 years. Long-term use of steroid sparing agents may protect against subclinical vascular disease activity. TTE was a reliable screening modality for late aortic dilatation.
To cite this abstract in AMA style:
Sammel A, Ho Shon I, Moses D, Stacey F, Mathur G, Hillenbrand C, Hsiao E, Geoffrey S, Laurent R, Wegner E. Aortic Dilatation and PET/CT Vascular Activity at Diagnosis and 5 Years in an Inception Giant Cell Arteritis (GCA) Cohort [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/aortic-dilatation-and-pet-ct-vascular-activity-at-diagnosis-and-5-years-in-an-inception-giant-cell-arteritis-gca-cohort/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/aortic-dilatation-and-pet-ct-vascular-activity-at-diagnosis-and-5-years-in-an-inception-giant-cell-arteritis-gca-cohort/