Session Information
Session Type: Poster Session B
Session Time: 8:30AM-10:30AM
Background/Purpose: In idiopathic inflammatory myopathies (IIM), SSa/SSb and Ro52 antibodies are frequently reported, especially in association with interstitial lung disease (ILD). However, limited literature exists on their prognostic role and use in risk assessment. The aim of this analysis was to describe ILD spectrum and pulmonary function tests (PFTs) in IIM patients in relation to anti-SSa/SSb and anti-Ro52 positivity.
Methods: We queried the Northwell Myositis Center database for patients with IIM between 1/1/2007 to 4/6/2018. Patients were selected if they met 2017 European League Against Rheumatism /American College of Rheumatology classification criteria for IIM and had anti-SSa/SSb data available. Results of commercially available anti-SSa/SSb and anti Ro52 immunoassays were used. Anti-SSb was only found in association with anti-SSa in this cohort and anti-SSa/SSb were combined and analyzed as a single group. ILD was defined by the presence of NSIP, COP/BOOP, UIP and unspecified ILD patterns on CT chest. PFTs variables were collected. Statistical analyses included Chi-square, Fisher’s Exact test, and Wilcoxon Rank Sum test to determine statistical differences in group distributions and McNemar’s test was performed to compare groups.
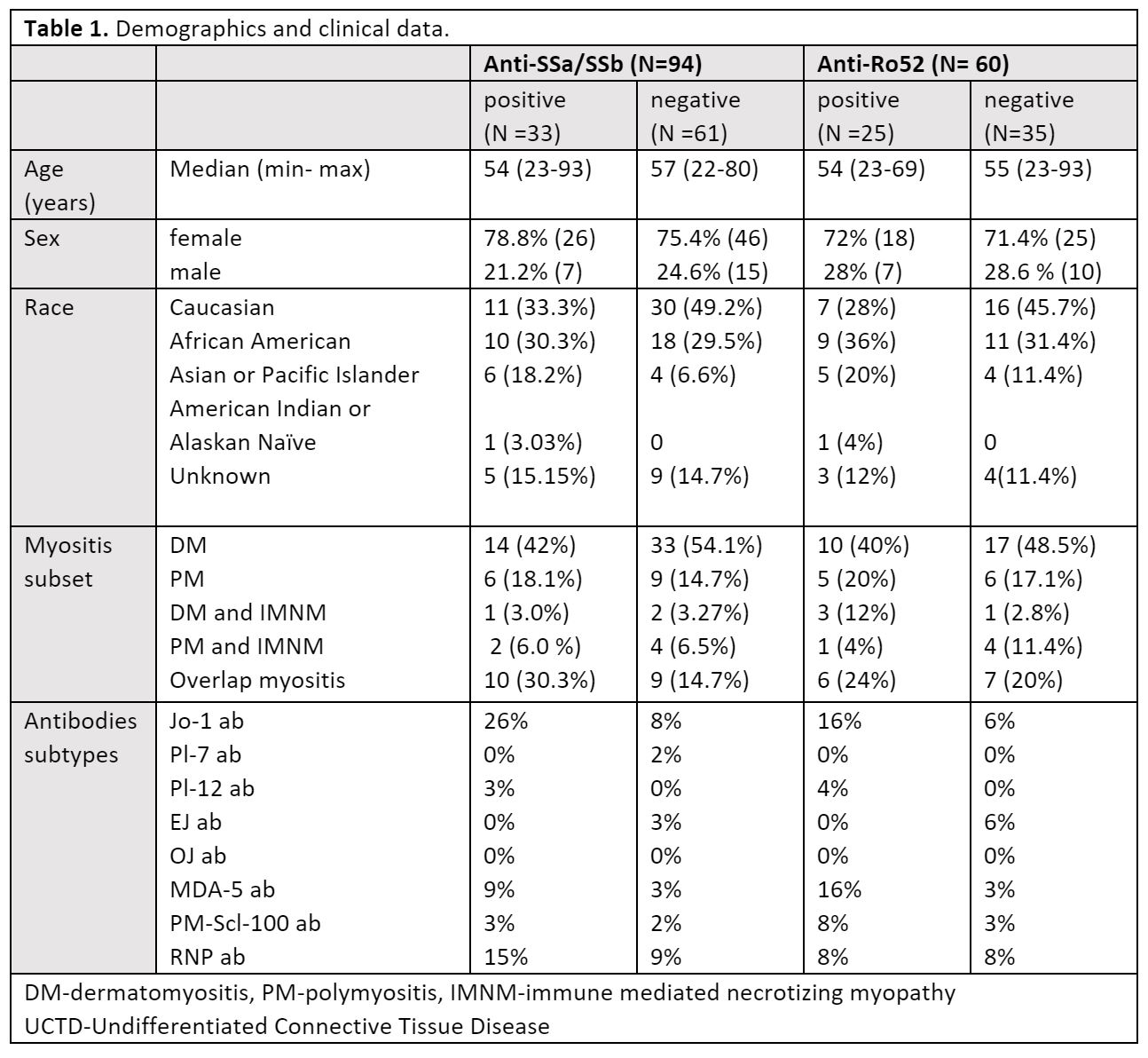
Results: 118 IIM adult (age > 18) patient records were reviewed. 15 with no anti-SSa/SSb and anti-Ro52 data and 9 anti-SSa/SSb negative patients with low positive Ro52 antibodies were excluded. Of 94 patients included in the analysis 35.1% (33 /94) were anti-SSa/SSb positive. Of 60 patients with available anti-Ro 52 41.6% % (25/60) were positive. The anti-SSa/SSb positive (n=33) and negative (n=61) groups and anti-Ro52 positive (n=25) and negative (n=35) groups had similar distribution for age, gender, and race, as well as subtypes of IIM. Demographics, clinical characteristics are listed in Table1.
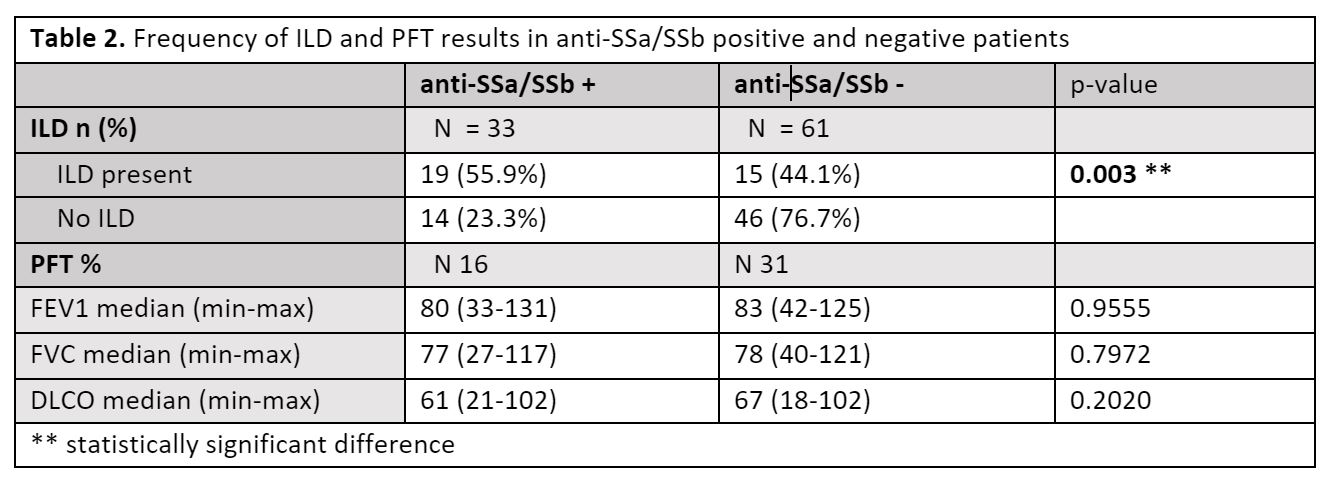
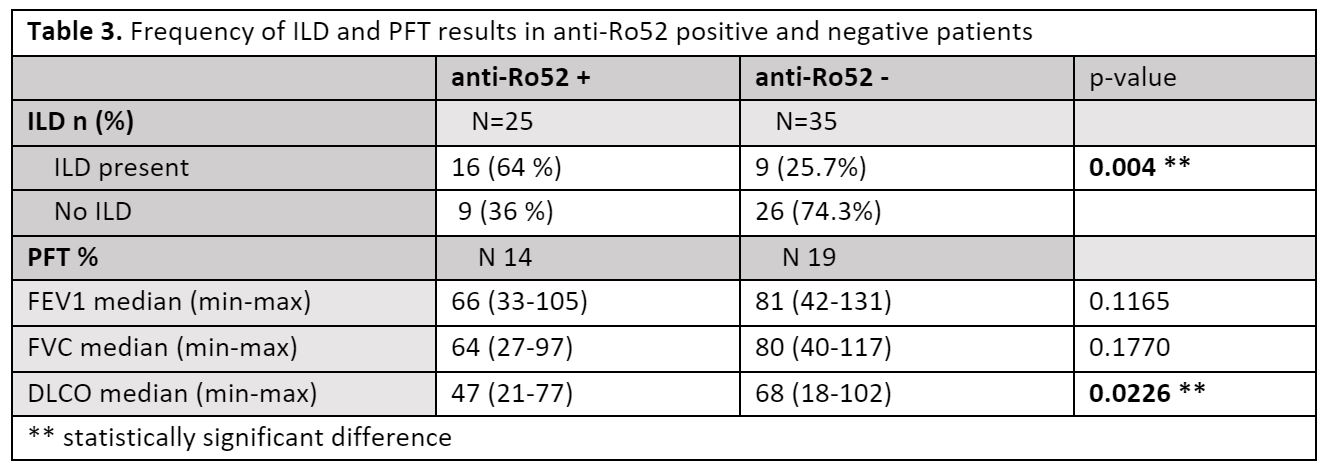
56% of patients with anti-SSa/SSb positive IIM had ILD compared to 44% of patient with negative anti-SSa/SSb (p = 0.003) regardless of anti-Ro52 status. 64% of patients with positive anti-Ro52 had ILD as compared with 36% of patient with negative anti-Ro52 (p= 0.004). NSIP and non-specified ILD were most reported irrespective of serological status, UIP was only seen in anti-SSa/SSb negative group. There was no statistically significant difference observed in FEV1, FVC, or DLCO between anti-SSA positive and anti-SSa negative patients. Interestingly, patients with positive Ro52 antibodies had a lower DLCO (47% vs. 68%; p = 0.003) than in anti-Ro52 negative patients, while there was no difference in FEV1 and FVC between groups.
Conclusion: While anti-SSa/SSb positivity is associated with higher rate of ILD, independent of anti-Ro 52 status, it does not confer an increased risk of ILD severity as measured with PFTs. DLCO in anti-Ro52+ group was significantly lower than that in anti-Ro52- group, indicating that anti-Ro 52 positivity is likely more applicable in predicting ILD severity than anti-SSa/SSb. This suggests that while both assays are useful in defining risk for ILD, anti-Ro52 is superior to the anti-SSa/SSb in determining severity of ILD in myositis patients.
To cite this abstract in AMA style:
Narain S, Valle A, Barilla-Labarca M, Marder G. Anti-SSa/SSb and Ro52 and Interstitial Lung Disease in Idiopathic Inflammatory Myopathies [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/anti-ssa-ssb-and-ro52-and-interstitial-lung-disease-in-idiopathic-inflammatory-myopathies/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/anti-ssa-ssb-and-ro52-and-interstitial-lung-disease-in-idiopathic-inflammatory-myopathies/