Session Information
Date: Monday, November 9, 2020
Title: Vasculitis – Non-ANCA-Associated & Related Disorders Poster II
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: Angiography is essential to detect vascular disease in patients with large-vessel vasculitis (LVV). Guidelines differ on the role of periodic angiography to monitor patients with LVV, in part due to limited prospective data regarding the natural history of angiographic disease. The objective of this study was to characterize angiographic progression of disease over time in Takayasu’s arteritis (TAK) and giant cell arteritis (GCA).
Methods: Patients with GCA or TAK were recruited into a prospective, observational cohort. All patients underwent baseline magnetic resonance (MR) or computed tomography (CT) angiography and a follow-up study (same modality) at least one year after baseline per a standardized imaging protocol. Angiographic lesions, defined as stenosis, occlusion, or aneurysm, were evaluated by visual inspection in 4 segments of the aorta and 13 branch arteries by a single reader blinded to clinical status. On follow up angiography, the development of new lesions was recorded and existing lesions were characterized as improved, worsened, or unchanged. Change over time was evaluated at the patient level and within each individual arterial territory.
Results: 1162 arterial territories were evaluated from 70 patients with LVV (TAK=38; GCA=32). Baseline characteristics were as follows: Age [TAK=29.5 years (18.4-39.5), GCA=69.6 years (60.7-75.5)], Female gender [TAK=30 patients (79%), GCA=23 patients (72%)], Disease duration [TAK=2.2 years (0.6-5.5), GCA=0.7 years (0.1-2.6)], Active clinical disease [TAK=17 patients (45%), GCA=20 patients (63%)]. The median time from initial study to follow up study was 1.6 years (1.0-2.7).
At the patient level, there were 12 new arterial territories that developed in 9 (13%) patients and occurred more frequently in patients with TAK=8 than GCA=1; p=0.03. Sixty patients (86%) had ≥1 territory affected at baseline (TAK=33, GCA=27). Angiographic lesions improved in 17 (28.3%) patients, with greater frequency in TAK=13 than GCA=4; p=0.05. Lesions worsened in 6 (10%) patients with no differences between diseases (TAK=4, GCA=2). In 7 (11.7%) patients (TAK=6, GCA=1), specific arterial territories improved while other territories worsened over follow up within the same patient.
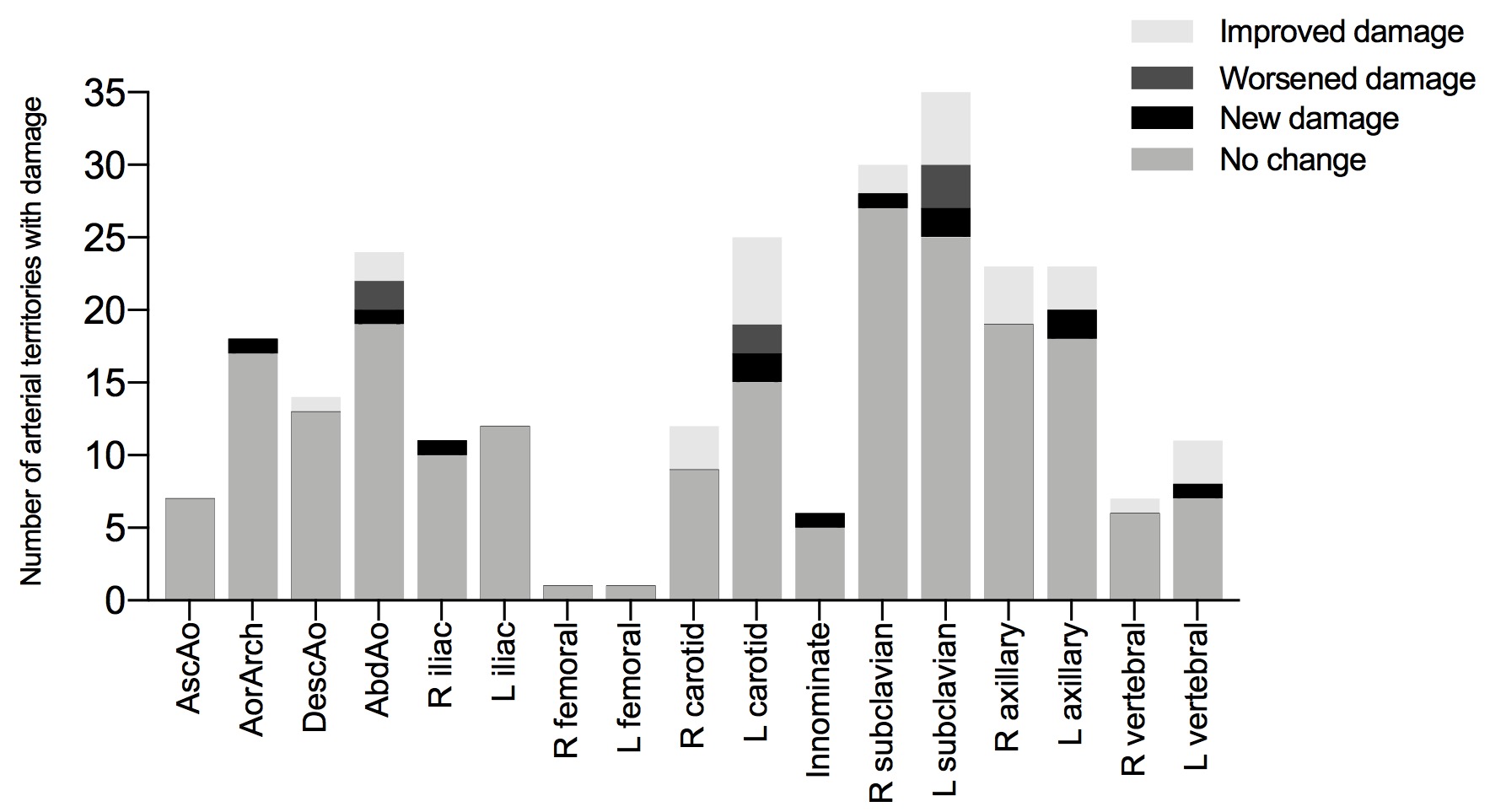
At the arterial territory level, 248 territories were affected at the baseline visit (TAK=145 territories, GCA=103 territories). At follow up, existing arterial lesions improved in 30 (12.1%) territories, worsened in 7 (2.8%) territories, and stayed the same in 211 (85.1%) territories. There were no significant differences in angiographic progression of disease at the territory level between GCA and TAK. Change in the branch arteries was more dynamic than change in the aorta (Figure).
Conclusion: Dynamic change in arterial lesions is observed in patients with TAK and GCA. Development of new angiographic lesions is infrequent and occurs more often in patients with TAK. Arterial lesions do not necessarily represent permanent damage, as a substantial number of lesions can improve. Discordant areas of improvement and worsening can occur within the same patient. These data may inform guideline recommendations for imaging monitoring in LVV.
To cite this abstract in AMA style:
Quinn K, Dashora H, Ahlman M, Novakovich E, Grayson P. Angiographic Progression of Disease in Large-Vessel Vasculitis [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/angiographic-progression-of-disease-in-large-vessel-vasculitis/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/angiographic-progression-of-disease-in-large-vessel-vasculitis/