Session Information
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: Systemic lupus erythematosus (SLE) is a multisystem condition that occurs more frequently in certain racial groups, particularly in populations of African ancestry. Low white blood cell counts (leucopenia) affect approximately 50% of patients with systemic lupus erythematosus (SLE) and often correlates with active disease. A variant in the ACKR1 promoter region (rs2814778-C) that is associated with neutropenia of no clinical significance is common among populations of African (AA) but not European ancestry (EA). We examined the hypotheses that: 1) leucopenia is more frequent in AA than EA patients with SLE, and 2) that the ACKR1 genotype rs2814778-CC accounts for the higher frequency of leucopenia in AA patients.
Methods: We performed a retrospective cohort study at a tertiary care system in EA (n=574) and AA (n=190) patients with SLE who had genetic and electronic health record (EHR) data. Ancestry was defined by principal components (PCs) and HapMap reference. White blood cell (WBC) and platelet counts after the first diagnosis code for SLE were extracted; leucopenia was defined as a WBC count < 4,000 cells/mm3 and thrombocytopenia as a platelet count < 100,000 cells/mm3. Genotyping was performed using the Illumina Infinium® Expanded Multi-Ethnic Genotyping Array. The ACKR1 SNP — rs2814778 C/T—was directly genotyped. Only the CC genotype is associated with lower neutrophil counts; thus, patients with TT and TC genotypes were compared to those with CC genotype. We examined the association of CC genotype with platelet count as differences in WBC counts by genotype may be confounded by other SLE-related factors (e.g., disease activity or medications).
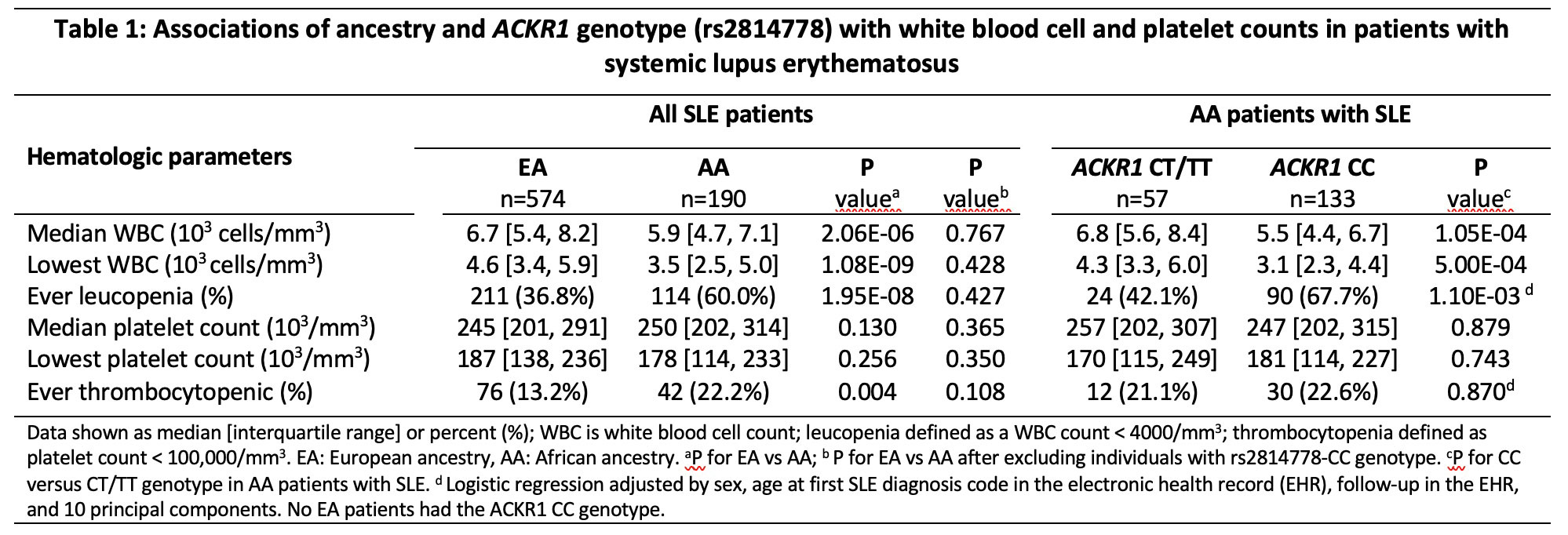
Results: The mean age at first diagnosis of SLE in the EHR was 42.3 (SD=16.6) years; patients were predominantly female (89%), and 25% were of AA. The median and lowest WBC counts were lower in AA than EA patients, and over a mean of 7.6 (5.6) years of follow-up, the rate of leucopenia was 60.0% in AA and 36.8% in EA patients (OR=2.6, 95%CI: 1.8-3.6, P=3.26E-08) (Table 1). The rs2814778-CC genotype was absent among EA patients but present in 70% of AA patients and was associated with lower WBC counts and more frequent leucopenia (OR=3.9, 95%CI: 1.7-8.9, P=0.001). The race differences observed in median WBC, lowest WBC, and rate of leucopenia were no longer significant after excluding AA individuals with the rs2814778-CC genotype (Table 1). Thrombocytopenia was more frequent in AA (22.1%) than EA (13.2%) patients, but in AA patients rs2814778-CC genotype was not associated with thrombocytopenia (CC 22.6% vs CT/TT 21.1%, P=0.870).
Conclusion: In SLE, AA patients had lower WBC counts and higher rates of leucopenia and thrombocytopenia than EA patients. The differences in WBC measures were largely explained by the rs2814778-CC genotype; this genotype could drive disparities in cytotoxic drug initiation and dose regulation and potentially influence outcomes in clinical practice.
To cite this abstract in AMA style:
Chung C, Karakoc G, Gamboa J, Mosley J, Cox N, Stein M, Kawai V. Ancestry, ACKR1, and Leucopenia in Patients with Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/ancestry-ackr1-and-leucopenia-in-patients-with-systemic-lupus-erythematosus/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/ancestry-ackr1-and-leucopenia-in-patients-with-systemic-lupus-erythematosus/