Session Information
Date: Saturday, November 16, 2024
Title: Vasculitis – Non-ANCA-Associated & Related Disorders Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Takayasu arteritis (TAK) typically affects people between the ages of 20 and 40. However, disease onset can span across different age periods. Aim of this work is to evaluate the influence of age at disease onset on baseline clinical features and vascular involvement and on treatment strategies in patients with TAK.
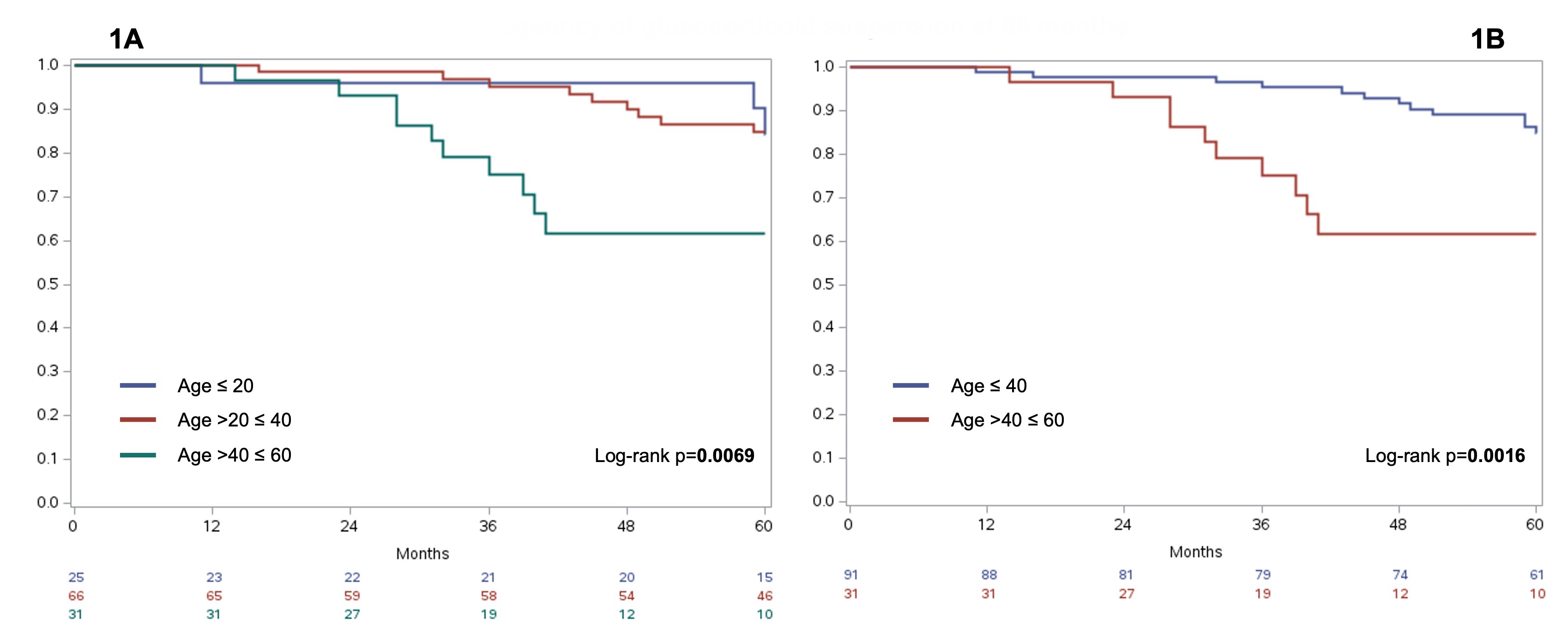
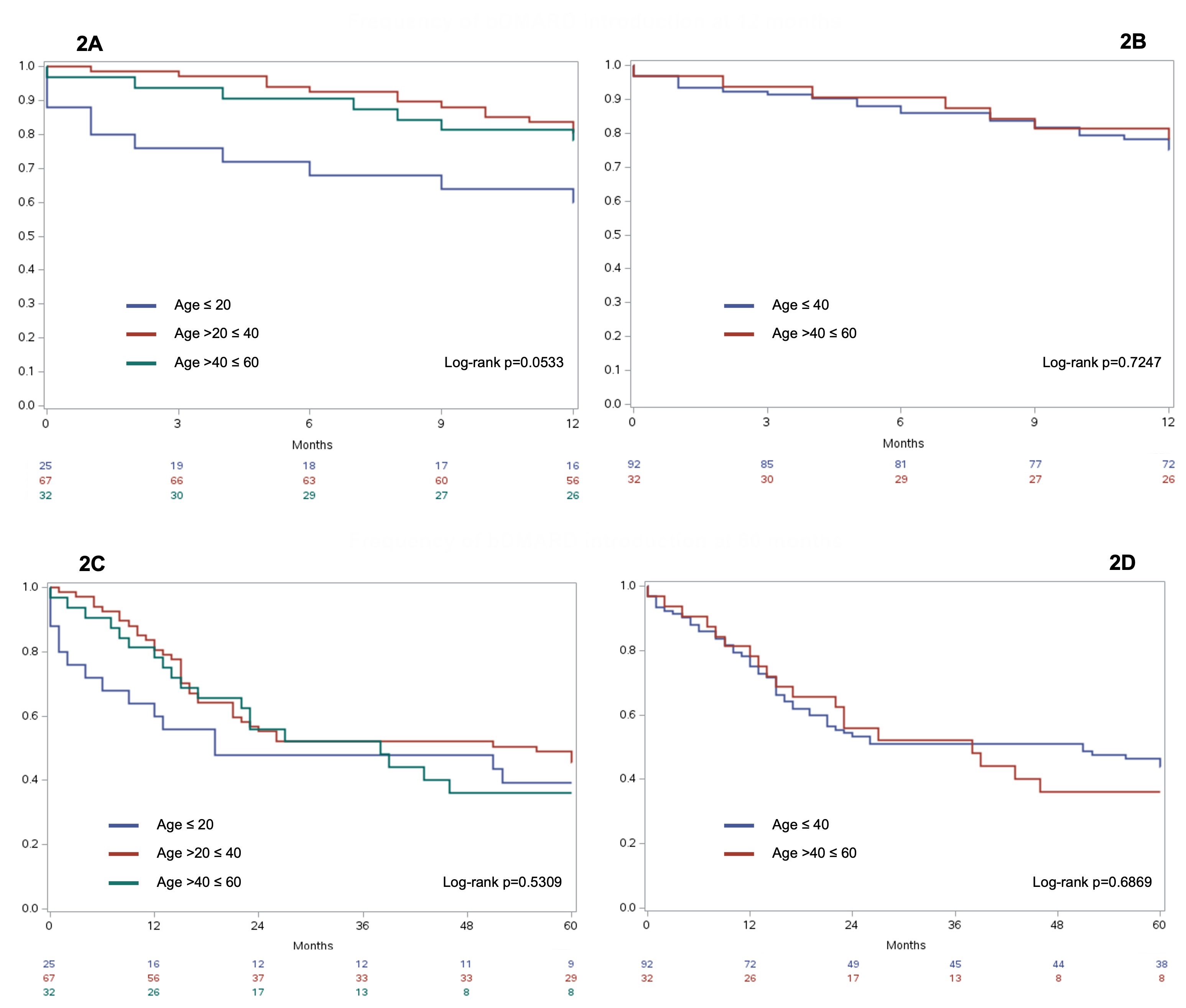
Methods: Medical records of TAK patients followed up at our Institution were retrospectively reviewed. Patients were divided according to the age at TAK onset first into 3 groups (A1, ≤20; A2, >20 and ≤40; B >40 and ≤60 years) and then into 2 groups (A ≤40; B >40 and ≤60 years). Diagnostic delay, fulfillment of the EULAR/ACR 2022 classification criteria, signs/symptoms and vessels involved at baseline were compared. In patients with a follow-up ≥12 months, treatment strategies (ie, glucocorticoid [GC] suspension and introduction of biologic agents [bDMARDs]) were evaluated at 12 and 60 months after diagnosis. Continuous variables were compared with the Mann-Whitney U or Kruskal-Wallis tests and categorical variables with the Chi-squared test. For the survival analyses, the Kaplan-Meier estimator and the log-rank test were employed. Two-sided p< 0.05 was considered statistically significant.
Results: Baseline features were available for 167 patients (A1, n=41[24%]; A2, n=83[50%]; A, n=124[75%]; B, n=43[26%]). In young patients there was a tendency to a longer diagnostic delay (A1, 19[3-48]; A2, 15[2-60]; A, 17[2-53]; B, 6[1-40] months). The mean ACR/EULAR classification criteria score was higher in young patients (A1, 9.8±2.6; A2, 9.7±3; B, 8.2±2.9; p=0.0165; A, 9.7±2.8; B, 8.2±2.9;p=0.0050); however, the % of patients meeting the criteria was comparable (A, 96%; A1, 98%; A2, 95%; B, 90%). Patients in group A suffered more frequently from syncope and upper limbs claudication than patients in group B (13% vs 0%, p=0.0132 and 40% vs 19%,p=0.0100). This difference was significative also when comparing the 3 groups (A1 22%, A2 8%, B 0%, p=0.0026 and A1 37%, A2 42%, B 19%,p=0.0299). Patients in group A had more frequently pulse loss/reduction in upper extremities and vascular bruits than patients in group B (64% vs 37%, p=0.0025 and 73% vs 51%,p=0.0100). These differences were significative also when comparing the 3 groups (A1 68%, A2 61%, B2 37%,p=0.0080; A1 73%, A2 73%, B 51%,p=0.0361). Patients in group B had more frequently involvement of abdominal aorta (A 44%, B 62%,p=0.0492), coronary (A 6%, B 24%,p=0.0018; A1 2%, A2 8%, B 24%,p=0.0045) and iliac arteries (A 14%, B 30%,p=0.0150). Outcome data were available for 124 patients (A1, n=25[20%]; A2, n=67[54%]; A, n=92[74%]; B, n=32[26%]). Age >40 years was associated with GC suspension at 60 months (Fig.1A-B); only 1 patient stopped GC during the first 12 months, so the analysis was not performed. No age group was associated with bDMARD start, but a trend for more frequent bDMARD inititation at 12 months in patients ≤20 was found (Fig.2A-D).
Conclusion: In a quarter of patients, TAK onset was after 40 years, highlighting the importance of maintaining high vigilance even in this age group. Patients with onset >40 years were less likely to have classic presentation and pattern of vascular involvement, appeared to have a less aggressive course and were easier to withdraw from GC.
To cite this abstract in AMA style:
Tomelleri A, Campochiaro C, Baldissera E, Farina N, Matucci-Cerinic M, Dagna L. Age at Disease Onset Influences the Clinical Phenotype and Outcome of Patients with Takayasu Arteritis: Results from a Monocentric Cohort of 167 Patients [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/age-at-disease-onset-influences-the-clinical-phenotype-and-outcome-of-patients-with-takayasu-arteritis-results-from-a-monocentric-cohort-of-167-patients/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/age-at-disease-onset-influences-the-clinical-phenotype-and-outcome-of-patients-with-takayasu-arteritis-results-from-a-monocentric-cohort-of-167-patients/