Session Information
Session Type: ACR Concurrent Abstract Session
Session Time: 11:00AM-12:30PM
Background/Purpose: While, a Treat-to-Target strategy (T2T), treating patients with rheumatoid arthritis (RA) towards a certain target (eg. clinical remission; T2T-REM), is highly recommended, several patients in clinical remission often have residual synovitis on ultrasound-imaging (US). This may result in silent radiographic progression and clinical flare. It is arguable whether targeting US-synovitis may result in ‘deeper’ remission in clinical practice. We aimed to assess whether using US in a T2T strategy leads to more patients meeting clinical remission than using only clinical information.
Methods: Patients with RA who started or changed csDMARD and/or anti-TNF treatment followed in centers with expertise in US and participating in BIODAM (2-year multicenter prospective observational cohort) were included. Clinical and US data [by the US7-score that includes 7 joints of the clinically dominant hand and foot for synovitis and tenosynovitis on gray-scale US (GSUS) and power-doppler US (PDUS) and erosions on GSUS] were collected every 3 months. Per visit and per protocol was decided whether the patient was treated according to the clinical definition of T2T with DAS44 remission as benchmark (T2T-DAS44). Though not mandatory, US-data could also be used for this purpose. T2T-DAS44 was considered correctly applied if: either i) a patient already had a disease activity score below the remission target (i.e. DAS44 remission) or ii) if not, treatment was intensified. A T2T strategy taking also US data into account (T2T-DAS44-US) was considered correctly applied if: either i) both DAS44 and US remission (all joints included in the US7-score with GSUS synovitis <2 and PDUS synovitis=0) were present; or ii) if not, the treatment was intensified. The main outcome was DAS44 remission. The effect of adding US to T2T (T2T-DAS44-US) on clinical remission 3 months later compared to a clinical remission benchmark only (T2T-DAS44) was analyzed using generalized estimating equations.
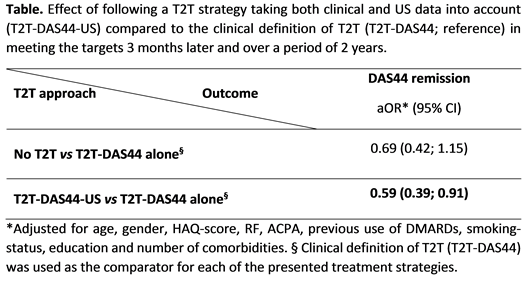
Results: In total 1,028 visits of 130 patients were included. T2T-DAS44-US was correctly followed in 41% of the visits, T2T-DAS44 in 23%, and any of these in 36%. Remission according to the DAS44 definition was achieved in 39% of the visits. Compared to the conventional T2T-DAS44 strategy, using a combined clinical and US benchmark for T2T led to a 40% lower – instead of higher – likelihood of DAS44 remission 3 months later [OR (95%CI): 0.59 (0.39; 0.91)(table).
Conclusion: Our results, from a non-randomized study, did not suggest an advantage of using US of 7 joints in addition to clinical examination as a T2T benchmark as compared to clinical examination alone in getting RA patients into clinical remission.
To cite this abstract in AMA style:
Sepriano A, Ramiro S, Landewé RBM, van der Heijde D, Ohrndorf S, FitzGerald O, Backhaus M, Larche M, Homik J, Saraux A, Hammer HB, Terslev L, Østergaard M, Burmester GR, Combe B, Dougados M, Hitchon CA, Boire G, Lambert RG, Dadashova R, Paschke J, Hutchings E, Maksymowych WP. Adding Ultrasound to the Treat-to-Target Strategy Shows No Benefit in Achievement of Remission: Results from the Biodam Cohort [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/adding-ultrasound-to-the-treat-to-target-strategy-shows-no-benefit-in-achievement-of-remission-results-from-the-biodam-cohort/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/adding-ultrasound-to-the-treat-to-target-strategy-shows-no-benefit-in-achievement-of-remission-results-from-the-biodam-cohort/