Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
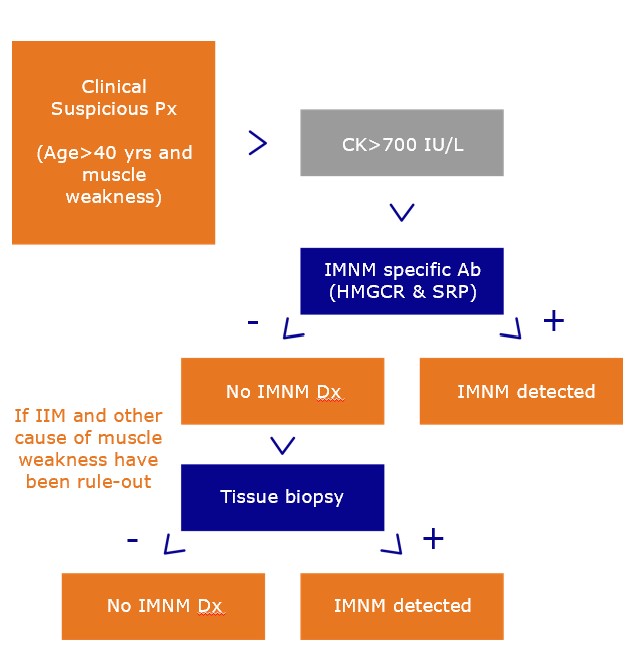
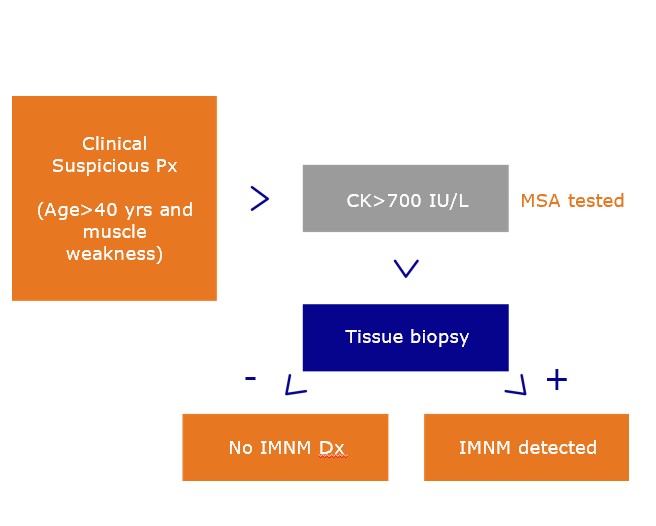
Background/Purpose: Immune-mediated necrotizing myopathies (IMNM) is a subgroup of immune-mediated myopathies (IMM). The diagnosis of IMNM relied on the presence of proximal muscle weakness, high levels of creatinine kinase (CK) and myofiber necrosis assessment through muscle biopsy. In 2018, the European Neuromuscular Centre (ENMC) recommended running anti-HMGCR and anti-SRP tests on patients with suspected IMNM and if the results were negative, then patients will undergo muscle biopsy for a diagnostic confirmation. Clinical practice is moving gradually towards ENMC diagnosis criteria, but no economic analysis has been done yet. This study assessed the economic consequences of following the ENMC guidelines through a cost-effectiveness analysis of IMNM when specific biomarkers are added in the diagnostic algorithm.
Methods: A decision tree model was designed to simulate a 1,000 hypothetical cohort of patients ≥40 years old with proximal muscle weakness and elevated creatine kinase levels under two interventions: 1) anti-HMGCR + anti-SRP + muscle biopsy (in seronegative cases); and 2) direct muscle biopsy (assumed as current clinical practice). Model parameters were derived from systematic literature review. The prevalence of IMNM was 8% based on a secondary care setting US study. Health related quality of life parameters were measured through utilities of phlebotomy and muscle biopsy. Direct medical costs were standardized to 2022 US dollars (therefore, this analysis did not include patient cost e.g., transport to the healthcare center, loss of productivity). Sensitivity analyses were conducted to assess changes in model output by varying several input data.
Results: The serological intervention was associated with a decreased of 79 muscle biopsies. Therefore, the cost per IMNM correctly diagnosed decreased by 83% ($2001). The cost per suspected IMNM patient decreased $160. Quality of life parameter is 8% higher in the serological intervention compared to the biopsy intervention. Results were sensitive to the IMNM prevalence, and the cost of biopsy and serological tests. In a clinical setting with a 1% IMNM prevalence, the cost-effective alternative is muscle biopsy, unless its cost is above $2,400 and the anti-HMGCR test cost is between $10-$15. At an 8% prevalence the serological intervention is more cost-effective unless the anti-HMGCR test cost is above $35 and cost of biopsy is above $600. At prevalence ≥19% the serological intervention is dominant at any anti-HMGCR test cost and muscle biopsy cost.
Conclusion: Our findings suggest that adding anti-HMGCR and anti-SRP test in the diagnostic algorithm of inflammatory idiopathic myopathies, as recommended by ENMC, results in less invasive diagnostic procedures a therefore having patients with a higher quality of life, at a lower cost. Confirmation of these economic results using real-world data is warranted.
To cite this abstract in AMA style:
Figueroa-Lara A, Aure M, Andalucia C. Added Value of Anti-HMGCR and Anti-SRP Antibodies in the Diagnosis of Immune Mediated Necrotizing Myopathy: An Outcome and Cost Comparison from the USA Perspective [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/added-value-of-anti-hmgcr-and-anti-srp-antibodies-in-the-diagnosis-of-immune-mediated-necrotizing-myopathy-an-outcome-and-cost-comparison-from-the-usa-perspective/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/added-value-of-anti-hmgcr-and-anti-srp-antibodies-in-the-diagnosis-of-immune-mediated-necrotizing-myopathy-an-outcome-and-cost-comparison-from-the-usa-perspective/