Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Patients with inflammatory arthritis (IA) report reduced physical activity and poor sleep, However, much remains unknown about the extent and impact of this relationship. Using accelerometry data from the NIH All of Us Research Program, we investigated (1) physical activity and sleep patterns in those with and without IA, and (2) the association of activity and sleep with risk of incident IA.
Methods: Participants who consented to share electronic health records and had at least one year of Fitbit accelerometry data in All of Us were included. IA was defined as ICD-10 codes for rheumatoid (RA) or psoriatic arthritis (PsA). Incident IA was defined as new IA diagnosis from the completion of accelerometry data up to 10 years. Daily step count, weekly moderate-vigorous physical activity (MVPA), daily sedentary time, and nightly sleep duration were assessed. Between group differences were tested using Kruskal-Wallis and Bonferroni-adjusted Dunn’s tests. Associations between accelerometry metrics with incident IA were identified using Cox proportional hazards models adjusting for age, sex, and race/ethnicity.
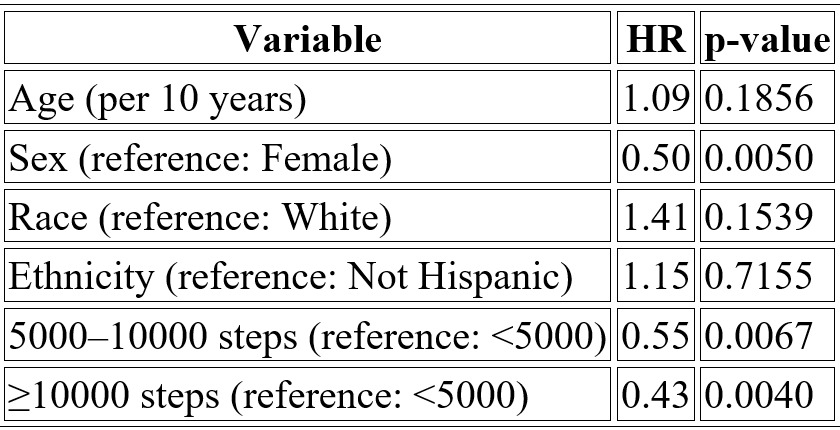
Results: 24,808 individuals were included (mean age 51.9 [15.3] years, 70% female, 79% White); 206 had IA (177 with RA and 29 with PsA). Compared to those without IA, participants with IA were older (58.0 vs 51.8 years, p< 0.001), female (81.6% vs 69.5%, p< 0.001), and had higher rates of hypertension (84.0% vs 32.6%, p< 0.001) and diabetes (41.3% vs 12.8%, p< 0.001). Participants with IA had lower median daily step counts (6,742 [5,093–9,327] vs 7,360 [5,386–9,693]; p< 0.001), lower weekly MVPA (147.0 [62.7–271.2] vs 185.3 [88.8–330.9] minutes; p< 0.001), and higher sedentary time (900.7 [759.3–981.3] vs 799.0 [704.8–961.1] minutes; p< 0.001). Sleep duration was similar between the two groups (371 [312, 418] vs 385 [332, 426] minutes; p=0.78).125 individuals developed incident IA. Adjusting for age, sex, and race/ethnicity, each additional 1,000 steps/day was associated with an 8% lower risk of IA (HR 0.92; p=0.012). Compared to < 5,000 steps/day, 5,000–10,000 steps/day was associated with a 45% lower risk (HR 0.55; p=0.007) and >10,000 steps/day with a 57% lower risk (HR 0.43; p=0.004). MVPA showed that participants engaging in ≥300 minutes/week of MVPA had a significantly lower risk of IA (HR 0.27; p=0.022) compared to those with < 30 minutes/week. There was no significant association between incident IA and sedentary time (HR 1.00 per minute; p=0.294) or nightly sleep duration (HR 1.04 per hour; p=0.388).
Conclusion: Accelerometers provide more objective and granular measurement of physical activity and sleep compared to self-reported data. Using 1-year accelerometry data from the NIH All of Us cohort, we observed lower physical activity and higher sedentary time in those with IA. Further, higher step counts and MVPA were significantly associated with reduced 10-year risk of incident IA, highlighting the crucial role of physical activity in IA prevention. Wearable technologies may offer valuable insights into the complex interplay between activity, sleep, and arthritis, and further studies in well-phenotyped cohorts are warranted.
 Cohort Characteristics
Cohort Characteristics
.jpg) Cox regression results showing the association between accelerometry-derived steps categorized by WHO guidelines and incident inflammatory arthritis.
Cox regression results showing the association between accelerometry-derived steps categorized by WHO guidelines and incident inflammatory arthritis.
.jpg) Kaplan Meier Survival Probability Curves for Categorical Steps and Categorical MVPA v Incident IA
Kaplan Meier Survival Probability Curves for Categorical Steps and Categorical MVPA v Incident IA
To cite this abstract in AMA style:
Kulkarni a, Scher J, Haberman R, Barua S. Accelerometry-Derived Activity and Sleep Patterns in the NIH All of Us Cohort: Insights and Predictive Potential for Inflammatory Arthritis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/accelerometry-derived-activity-and-sleep-patterns-in-the-nih-all-of-us-cohort-insights-and-predictive-potential-for-inflammatory-arthritis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/accelerometry-derived-activity-and-sleep-patterns-in-the-nih-all-of-us-cohort-insights-and-predictive-potential-for-inflammatory-arthritis/