Session Information
Date: Tuesday, October 23, 2018
Title: Metabolic and Crystal Arthropathies – Basic and Clinical Science Poster II
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose:
The safety of allopurinol in the setting of chronic kidney disease (CKD) has been a controversial issue for many years. The perceived increased risk of adverse reactions has made many providers hesitant to use allopurinol in the setting of CKD, leading to inadequate control of this highly prevalent malady. Rheumatologists are generally thought to endorse higher doses of allopurinol in CKD than nephrologists. As there is much overlap between the gout and CKD patient populations, this may lead to conflicting messages regarding allopurinol safety and dosing, which may threaten adherence to urate-lowering therapy. These differences may reflect an educational need or areas where improved communication between providers is important.
A script concordance test (SCT) for gout developed by Siaton et al has demonstrated evidence of validity including high reliability (Cronbach’s alpha = 0.93), large effect size (Cohen’s d = 0.90), and generalizability for use across multiple institutions and learner groups.1,2 This study aimed to use the SCT to explore differences between academic nephrologists and rheumatologists regarding the use of allopurinol in the setting of gout and CKD.
Methods:
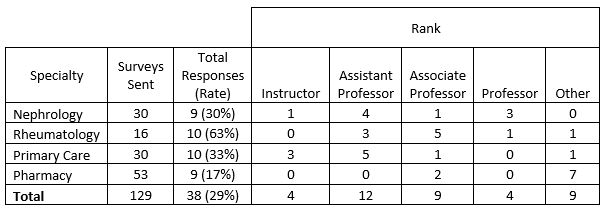
Using the REDCap online platform, questions from the SCT relevant to the treatment of gout with allopurinol in the setting of CKD were sent via e-mail to attending nephrologists, rheumatologists, primary care providers, and pharmacists associated with training programs of University of Utah. With Excel, response rates were calculated, descriptive statistics were analyzed, and significance of differences in mean responses between specialty groups were examined using 2-tailed Student’s t-test.
Results:
To date, 38 responses (29%) have been received; details are presented in the Table below:
Conclusion:
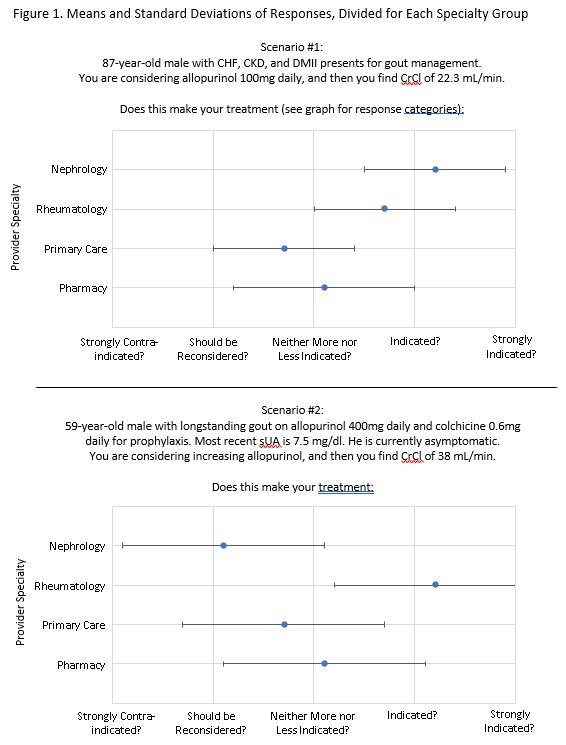
Nephrologists were more willing than rheumatologists to start allopurinol at a relatively high dose in CKD (100 mg daily), but were less likely to increase allopurinol to achieve a serum uric acid (sUA) target. This highlights what may be a fundamental disagreement on the mechanism and timing of allopurinol toxicity and the importance of achieving sUA target, where rheumatologists believe it is more dangerous when first being initiated, and nephrologists are less concerned about achieving target sUA in CKD.
References
1. Siaton BC, Clayton E, Kueider AM, Rietschel M. Arthritis Rheumatol. 2016; 68 (suppl 10).
2. Siaton BC, Barker A, Battistone MJ. Arthritis Rheumatol. 2017;69(suppl 10)
To cite this abstract in AMA style:
Lebedoff N, Gilligan S, Barker A, Koening CL, Starman K, Gallop C, Siaton BC, Raphael KL, Battistone MJ. A Validated Script Concordance Test Demonstrates Interdisciplinary Differences in Clinical Decision-Making When Using Allopurinol to Treat Gout in Chronic Kidney Disease [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/a-validated-script-concordance-test-demonstrates-interdisciplinary-differences-in-clinical-decision-making-when-using-allopurinol-to-treat-gout-in-chronic-kidney-disease/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-validated-script-concordance-test-demonstrates-interdisciplinary-differences-in-clinical-decision-making-when-using-allopurinol-to-treat-gout-in-chronic-kidney-disease/