Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose
Controversies exist regarding whether patients with osteoarthritis (OA) have an increased risk of cardiovascular (CV) disease. Our aim was to evaluate the CV risk in a population-based OA cohort.
Methods
The Musculoskeletal pain in Ullensaker STudy (MUST) is a cross-sectional investigation comprising a thorough clinical examination, recording of CV risk factors in addition to radiographic evaluation of hands, hips and knees of persons with self-reported OA (The MUST-Heart study). Of the 604 persons examined, 438 fulfilled the ACR classification criteria for OA in the hand, knee and/or hip joints. The study population was divided into: 1) generalized OA, defined as bilateral hand OA or involvement of > 3 out of 6 sites (bilateral hand/hip/knee); 2) focal OA; or 3) non-OA. CV risk was calculated by the SCORE algorithm for persons without CV disease, not using lipid lowering and/or antihypertensive medication (OA n=200 and non-OA n=87). An estimated CV risk < 5% for a fatal myocardial infarction coming 10 years is defined as low to medium risk, while > 5% is the cut off for initiation of CV preventive pharmacotherapy. Comparisons between groups were done by using independent samples T-test, Mann Whitney-U and χ2.
Results
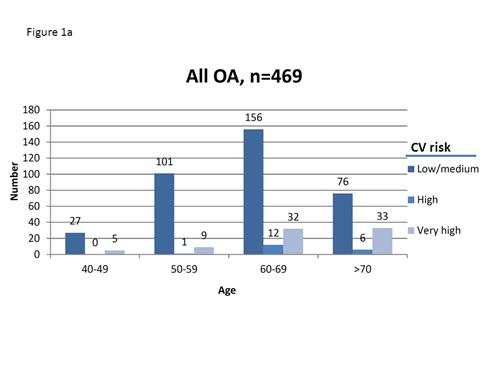
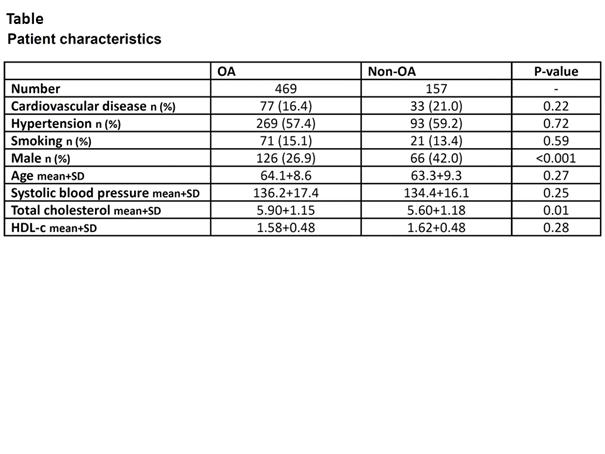
The median CV risk for patients with OA [1.40 (IQR 0.65, 2.92)] was significantly higher compared to non-OA [0.99 (IQR 0.52, 1.92)] (p=0.02). The difference in the CV risk was related to higher age (p <0.001), but not to total cholesterol (p=0.07), systolic blood pressure (p=0.13) or to the OA diagnosis. Only 17/200 (8.5%) of the OA patients and 3/87 (3.4%) of the non-OA persons had a CV risk > 5% (p=0.12) (Table). The presence of established CV disease was comparable for those with (n=72/438, 16.8%) and without OA (n=34/166, 21.1%) (p=0.23). Dividing the OA group into focal and generalized OA, did not reveal any further differences regarding estimated CV risk or CV disease compared with non-OA. Inflammatory biomarkers (erythrocyte sedimentation rate and C-reactive protein) were in the normal range for the whole study population, with no difference between OA and non-OA (p=0.30 and 0.10, respectively)(Fig 1a&b).
Conclusion
Inhabitants with OA in a Norwegian municipality had an overall low risk of CV disease and did not have higher prevalence of established CV disease compared to non-OA.

Disclosure:
S. Rollefstad,
None;
I. Eeg,
None;
I. K. Haugen,
None;
I. C. Olsen,
None;
N. Østerås,
None;
B. Christensen,
None;
H. B. Hammer,
None;
L. Nordsletten,
None;
B. Natvig,
None;
T. K. Kvien,
None;
A. G. Semb,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/patients-with-osteoarthritis-do-not-have-increased-risk-of-cardiovascular-disease-in-ullensaker-community-in-norway/