Session Information
Session Type: Abstract Submissions (ACR)
Treatment Patterns of Multimorbid Rheumatoid Arthritis Patients: Results from an International Cross-sectional Study
Background/Purpose
The presence of multimorbidity could lead to less intensive treatment of RA. This can increase RA disease activity and worsen outcomes such as function, quality of life and mortality.
The aim of the study is to describe the treatment profile of multimorbid RA patients in contrast to patients with RA only, and compare it across different international regions.
Methods
COMORA is a cross-sectional study assessing morbidities, RA related outcomes and treatment of RA patients, recruited in 17 countries worldwide. Patients were grouped according to their multimorbidity profile assessed by a counted multimorbidity index (cMMI), enumerating the particular number of morbidities for each patient. Treatment for RA was categorized according to the use of biologic DMARDs (bDMARD) and TNF-inhibitors (TNFi) in particular, use of synthetic DMARDs only (sDMARD), NSAID use and use of steroids for patients by their cMMI. Adjusted logistic regression models were examined to determine the odds ratio (OR) and 95% confidence interval (CI) of use of bDMARD, TNFi, sDMARD, NSAID or steroids, based on a patient’s cMMI and global region, after adjusting for age, disease activity, disease duration, and previous DMARD therapy.
Results
The study cohort consisted of 3920 patients, and 2563 (65.4%) were multimorbid. Overall, 92.6% of the patients were on DMARD therapy, 32.7% received bDMARD; 59.2% sDMARD only; 51.1% NSAIDs and 54.8% corticosteroids. Regional differences could be observed with the most frequent use of bDMARDs in US (46.5%) and lowest frequency in North Africa (9.0%) (Figure). After adjusting for confounders in logistic regression analyses, the OR for use of bDMARDs was reduced for each additional morbidity (OR 0.90, 95%CI 0.83-0.97). Similarly, the probability for use of TNFi was also reduced (OR 0.92, 95%CI 0.84-0.99), whereas the OR for use of sDMARD was increased (OR 1.12, 95%CI 1.04-1.21). No change of OR was found for NSAID or steroid use (Table).
Conclusion
In our cohort, differences in bDMARD prescribing exist across global regions. After adjusting for covariates, the OR of bDMARD and TNFi use decreases 10% for each additional chronic morbid condition as assessed by cMMI, whereas the OR of sDMARD use increased, probably reflecting rheumatologists’ greater comfort using these agents in patients with a greater multimorbidity burden.
Figure: Regional differences of current treatment status
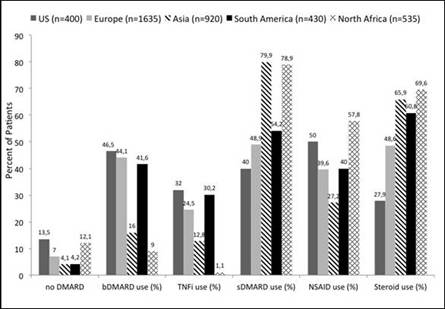
Table: Logistic regression models
|
Covariates
|
|
Odds Ratio (95% Confidence Interval)
|
|||
|
bDMARD
|
TNFi
|
sDMARD
|
NSAIDs
|
Steroids
|
|
|
Counted multimorbidity index |
0.90 (0.83-0.97)* |
0.92 (0.84-1.0)* |
1.12 (1.04-1.21)* |
1.06 (0.99-1.34) |
1.01 (0.98-1.13) |
|
Age (years) |
0.99 (0.98-1.0) |
0.99 (0.98-1.0) |
1.0 (0.99-1.01) |
0.98 (0.97-0.99)* |
1.0 (0.99-1.0) |
|
Disease duration (years) |
1.02 (1.0-1.03)* |
1.03 (1.01-1.04)* |
0.99 (0.98-1.0) |
1.01 (1.0-1.03)* |
1.0 (0.99-1.01) |
|
Number of previous DMARDs |
1.27 (1.18-1.37)* |
0.94 (0.87-1.02) |
0.71 (0.65-0.77)* |
1.05 (0.98-1.13)* |
1.21 (1.12-1.30)* |
|
Clinical disease activity index |
0.98 (0.97-0.99)* |
0.96 (0.95-0.97)* |
1.0 (0.99-1.01) |
1.03 (1.02-1.04)* |
1.04 (1.03-1.06)* |
|
Region US= reference |
REF |
REF |
REF |
REF |
REF |
|
Region Europe |
0.57 (0.38-0.85)* |
0.58 (0.39-0.85)* |
2.11 (1.35-3.27)* |
0.94 (0.65-1.37) |
2.50 (1.67-3.73)* |
|
Region Asia |
0.15 (0.10-0.23)* |
0.24 (0.15-0.39)* |
8.49 (5.23-13.6)* |
4.22 (2.74-6.50)* |
6.43 (4.10-10.1)* |
|
Region South America |
0.56 (0.34-0.94)* |
0.62 (0.37-1.06)* |
2.51 (1.46-4.37)* |
1.75 (1.06-2.90)* |
2.56 (1.52-4.33)* |
|
Region North Africa |
0.06 (0.03-0.11)* |
0.03 (0.01-0.08)* |
9.07 (5.34-15.4)* |
0.58 (0.37-0.92)* |
5.10 (3.09-8.35)* |
*p<0.05
Disclosure:
H. Radner,
None;
K. Yoshida,
None;
I. Hmamouchi,
None;
M. Dougados,
None;
J. Smolen,
None;
D. H. Solomon,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/treatment-patterns-of-multimorbid-rheumatoid-arthritis-patients-results-from-an-international-cross-sectional-study/