Session Information
Date: Tuesday, October 28, 2025
Title: Abstracts: ARP II: Perception, Prediction, and Prevention (2603–2608)
Session Type: Abstract Session
Session Time: 4:15PM-4:30PM
Background/Purpose: Metabolic dysfunction-associated steatotic liver disease (MASLD) is increasingly recognized as a cardiometabolic risk factor. Individuals with psoriasis have a high prevalence of MASLD, yet the association between MASLD and cardiac manifestations in this population remains unclear.
We aimed to evaluate associations between MASLD, cardiovascular risk factors, and cardiac structure and function in adults with psoriasis.
Methods: A total of 261 adults with psoriasis were consecutively enrolled in the PSOCADIA study (Prevalence and risk factors asSOciated with CArdiac comorbiDIty in psoriAsis, ClinTrials.gov: NCT04950218) from the Copenhagen Translational Skin Immunology Biobank and Research Programme (BIOSKIN). Participants underwent clinical assessment, transthoracic echocardiography, transient elastography (TE), and blood withdrawal. MASLD was defined as hepatic steatosis on TE with controlled attenuation parameter ³ 250 dB and presence of ³ 1 cardiometabolic risk factor(s), excluding other causes of liver disease. Measures of cardiac structure and function were compared between psoriasis patients with MASLD and those without MASLD. Associations between MASLD, diastolic and systolic dysfunction were assessed in uni- and multivariable regression models.
Results: We prospectively enrolled 261 individuals with psoriasis (median age 53.5 years, 46.4% women), whereof 20.7% had psoriatic arthritis. MASLD was present in 90 patients (34.5%) of whom 7 (8%) had possible advanced fibrosis. Compared to individuals without MASLD, those with MASLD exhibited higher blood pressure, higher body mass index (BMI), and more adverse cardiometabolic profiles including more prevalent diabetes (14.4% vs. 1.9%, p < 0.001). MASLD was associated with structural measures indicative of cardiac hypertrophy and worse measures of diastolic and systolic function. However, after adjusting for age, sex, and BMI, these associations were no longer statistically significant. In fully adjusted models, MASLD was not associated with diastolic or systolic dysfunction. In contrast, higher BMI and diabetes remained independently associated with myocardial dysfunction.
Conclusion: In adults with psoriasis, associations between MASLD and abnormal cardiac structure and function were attenuated after adjustment for cardiometabolic risk factors, underscoring the importance of risk factor control in individuals with psoriasis and concomitant MASLD. This may also reflect that most adults with psoriasis and MASLD did not have hepatic fibrosis in this cohort.
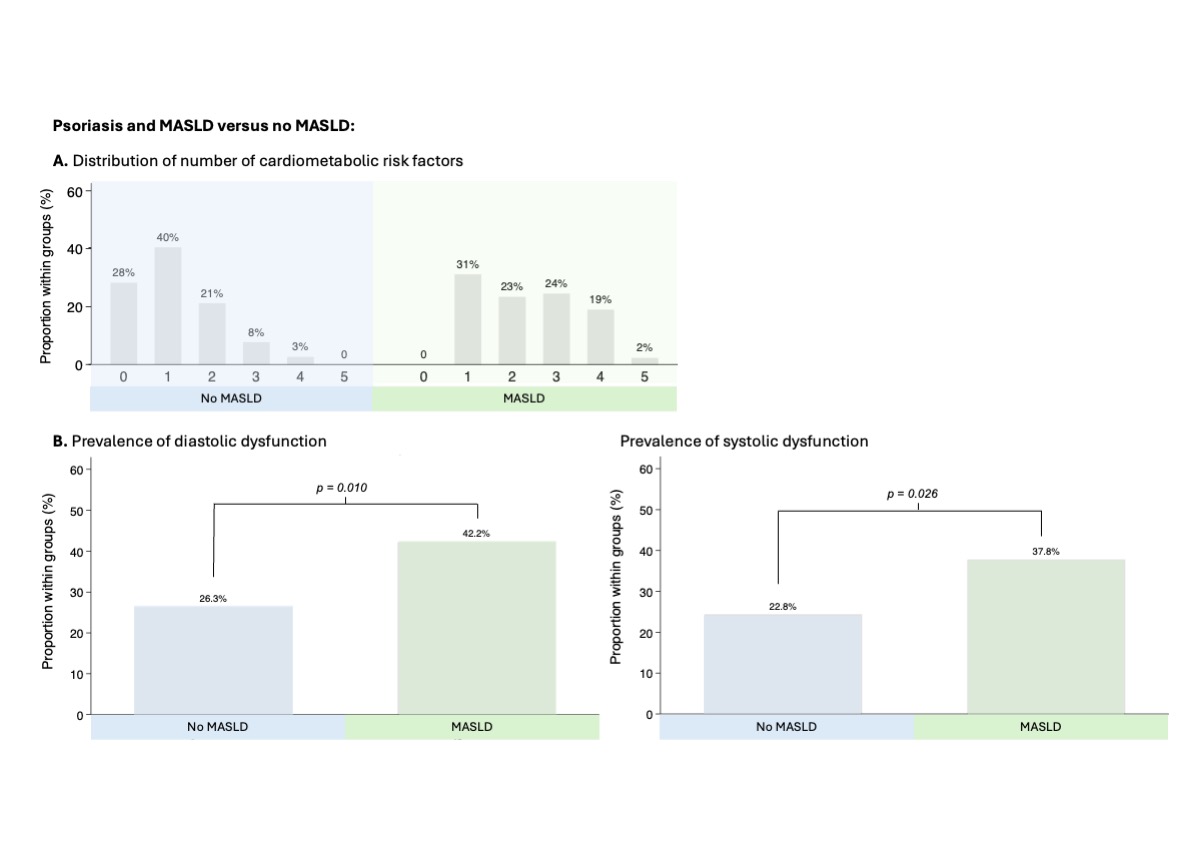 Cardiometabolic risk factors and myocardial dysfunction in adults with psoriasis with and without MASLD. A) Distribution of the number of cardiometabolic risk factors and B) Prevalence of diastolic and systolic dysfunction in individuals with psoriasis with and without MASLD. Bars represent the proportion of individuals (%) within each group. Cardiometabolic risk factors included obesity, hypertension, dyslipidemia, diabetes, and metabolic syndrome.
Cardiometabolic risk factors and myocardial dysfunction in adults with psoriasis with and without MASLD. A) Distribution of the number of cardiometabolic risk factors and B) Prevalence of diastolic and systolic dysfunction in individuals with psoriasis with and without MASLD. Bars represent the proportion of individuals (%) within each group. Cardiometabolic risk factors included obesity, hypertension, dyslipidemia, diabetes, and metabolic syndrome.
Abbreviations: MASLD, metabolic dysfunction-associated liver disease.
.jpg) Association between MASLD and cardiac structure and function in A) uni- and B) multivariable models adjusted for age, sex, and BMI. Mean differences (x-axis) in echocardiographic measures of cardiac structure, diastolic and systolic function (y-axis) in MASLD compared to no MASLD in the study population. Mean differences plotted with 95% confidence intervals in A) univariable linear regression models and B) multivariable linear regression models adjusted for age, sex, and BMI.
Association between MASLD and cardiac structure and function in A) uni- and B) multivariable models adjusted for age, sex, and BMI. Mean differences (x-axis) in echocardiographic measures of cardiac structure, diastolic and systolic function (y-axis) in MASLD compared to no MASLD in the study population. Mean differences plotted with 95% confidence intervals in A) univariable linear regression models and B) multivariable linear regression models adjusted for age, sex, and BMI.
Abbreviations: IVSd, Interventricular septum diameter; LVPWd, Left ventricular posterior wall diameter; LVMi, Left ventricular mass index; RWT, Relative wall thickness; LAVi, Left atrial volume index; MV E, Mitral valve early filling velocity; MV A, Mitral valve atrial contraction velocity; E/A, Ratio of early to late mitral inflow velocities; e’, Early diastolic mitral annular velocity; E/e’, Ratio of early mitral inflow to mitral annular velocity; TR Vmax, Tricuspid regurgitation peak velocity; LVEF, Left ventricular ejection fraction; GLS, Global longitudinal strain.
.jpg) Associations between MASLD, cardiometabolic risk factors and myocardial dysfunction in psoriasis. Uni- and multivariable associations between risk factors and diastolic and systolic dysfunction. Forest plots display odds ratios (OR) for diastolic dysfunction (left panels) and systolic dysfunction (right panels) on logarithmic scale with 95% confidence intervals for MASLD and other key cardiometabolic risk factors. Top panels show univariable models for each risk factor, while bottom panels show fully adjusted models for age, sex, and all risk factors.
Associations between MASLD, cardiometabolic risk factors and myocardial dysfunction in psoriasis. Uni- and multivariable associations between risk factors and diastolic and systolic dysfunction. Forest plots display odds ratios (OR) for diastolic dysfunction (left panels) and systolic dysfunction (right panels) on logarithmic scale with 95% confidence intervals for MASLD and other key cardiometabolic risk factors. Top panels show univariable models for each risk factor, while bottom panels show fully adjusted models for age, sex, and all risk factors.
Abbreviations: MASLD, metabolic dysfunction-associated steatotic liver disease; BMI, body mass index; MetS, metabolic syndrome.
To cite this abstract in AMA style:
Dons M, Näslund-Koch C, Sengeløv M, Bøgh-Sørensen S, Skaarup K, Løvendorf M, Davidovski F, Jensen A, Weber B, Gluud L, Zachariae C, Skov L, Biering-Sørensen T. Metabolic dysfunction-Associated Steatotic Liver Disease, Cardiometabolic Risk Factors, and Cardiac Manifestations in Psoriasis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/metabolic-dysfunction-associated-steatotic-liver-disease-cardiometabolic-risk-factors-and-cardiac-manifestations-in-psoriasis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/metabolic-dysfunction-associated-steatotic-liver-disease-cardiometabolic-risk-factors-and-cardiac-manifestations-in-psoriasis/