Session Information
Date: Tuesday, October 28, 2025
Title: Abstracts: ARP II: Perception, Prediction, and Prevention (2603–2608)
Session Type: Abstract Session
Session Time: 3:15PM-3:30PM
Background/Purpose: Current consensus for defining sarcopenia (loss of muscle mass and strength with aging) and sarcopenic obesity (SO, sarcopenia with obesity) suggests combining measures of strength and physical function with body composition parameters. Limited evidence suggests that SO is associated with knee osteoarthritis (KOA), moreso than either sarcopenia or obesity alone. However, previous studies often defined SO using only body composition or clinical measures, rather than a combination of both. Therefore, this study examined the relationship between KOA and sarcopenia, obesity, and SO utilizing a definition of sarcopenia, obesity, and SO that combined body composition and clinical definitions.
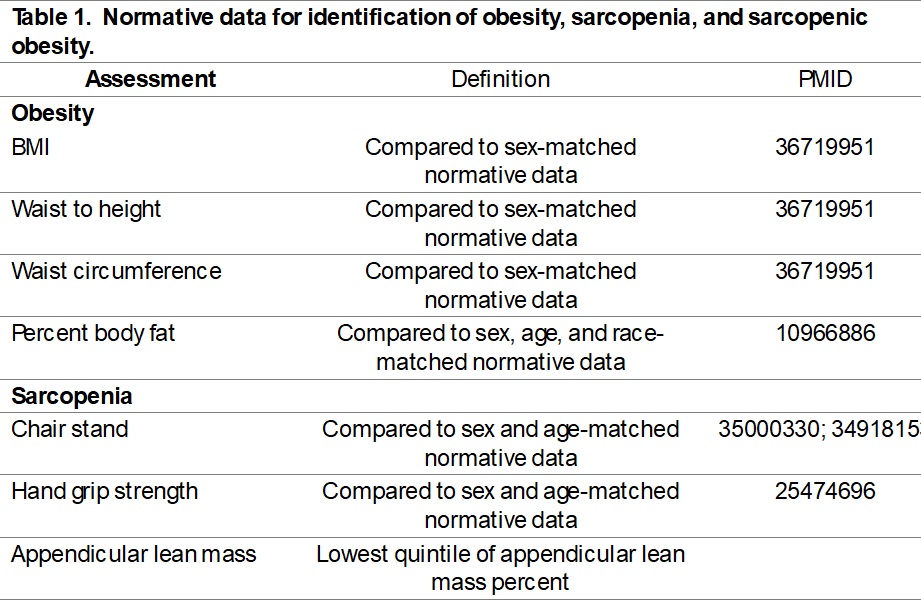
Methods: The sample was drawn from participants enrolled in the Johnston County Osteoarthritis Project (JoCoOA) with available whole body dual energy x-ray absorptiometry (DXA) scans, along with data on anthropometric, knee symptoms and radiographic, and physical function measures from one visit occurring between 1999-2010. Obesity was defined using cutoffs based on body fat % and either BMI, waist-to-height, or waist circumference (Table 1). Sarcopenia was defined as low fat-free mass with either low grip strength or poor chair stand time when compared to age and sex-matched normative values (Table 1). SO was defined as having both obesity and sarcopenia. Outcomes included radiographic KOA (rKOA) defined by a Kellgren-Lawrence grade ≥2 and symptomatic knee OA (sxKOA) defined by rKOA and symptoms (pain, aching, stiffness on most days) in the same knee. Logistic regression models assessed cross-sectional associations among obesity, sarcopenia, and SO and rKOA or sxKOA, adjusting for age, sex, race (Black/White), education level, smoking status(never/former/current), number of chronic conditions, and prior knee injury.
Results: A total of 1878 participants (mean age 63.6±10.4 years, 1/3 male, 1/3 Black) were included (Table 2). Individuals were classified as having neither obesity nor sarcopenia (64%), obesity only (23%), sarcopenia without obesity (2%), and SO (10%). Approximately 1/3 of the sample had rKOA and 2/5 had sxKOA. Compared to the referent group of no obesity or sarcopenia, obesity only and SO were associated with more than double the odds of rKOA and sxKOA (Table 3). Compared to obesity only, SO was related to sxKOA but not rKOA, and compared to sarcopenia only, SO was associated with rKOA and sxKOA.
Conclusion: These findings suggest that SO is strongly related to sxKOA when compared to obesity only or normal cutoffs of fat-free and fat mass. Both sarcopenia and obesity are related to changes in body composition and metabolic function associated with aging and the combination of sarcopenia and obesity (i.e. SO) works synergistically in its relationship with KOA, as the odds are higher than both conditions in isolation. Future research using current definitions of SO should investigate longitudinal relationships to inform interventions to address SO and KOA.
.jpg)
.jpg)
To cite this abstract in AMA style:
Werner D, Alvarez C, Batsis J, Blay R, Bilek L, Nelson A, Golightly Y. Cross-Sectional Relationship Between Sarcopenic Obesity and Knee Osteoarthritis: The Johnston County Osteoarthritis Project [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/cross-sectional-relationship-between-sarcopenic-obesity-and-knee-osteoarthritis-the-johnston-county-osteoarthritis-project/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cross-sectional-relationship-between-sarcopenic-obesity-and-knee-osteoarthritis-the-johnston-county-osteoarthritis-project/