Session Information
Date: Tuesday, October 28, 2025
Title: (2524–2546) Vasculitis – Non-ANCA-Associated & Related Disorders Poster III
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: IgG4-related disease (IgG4-RD) is a chronic immune-mediated disease characterized by mass-forming fibrotic lesions. The aim of this work was to characterize the overall clinical and serological findings of paravertebral (PV) and ureteropelvic junction (UPJ) involvement as two uncommon manifestations that are nevertheless regarded as strongly suggestive of IgG4-RD.
Methods: Patients with IgG4-RD were recruited from the Massachusetts General Hospital (MGH) Rheumatology Unit from 2008 to 2025. All patients included fulfilled the 2019 ACR/EULAR Classification Criteria for IgG4-RD. The presence of a PV or UPJ mass was determined by chart and imaging review. Demographics, age at diagnosis, organ involvement, and laboratory values were extracted from the medical record. Patients with PV or UPJ masses were compared to all other IgG4-RD patients in the registry.
Results: Among the 400 patients who fulfilled classification criteria in the MGH IgG4-RD registry, 7 (2%) had a PV mass and 11 (3%) had a UPJ mass. No patient had masses in both the PV and UPJ regions. PV masses were typically located anterolateral to the thoracic spine, abutting the vertebral bodies, and forming a band-like structure (Figure 1A). UPJ masses were typically extrinsic to the kidney and abutting the renal vasculature and ureter but generally not causing hydronephrosis (82%, only two patients presented with hydronephrosis one of whom with concomitant retroperitoneal fibrosis) (Figure 1B). All 7 patients with PV masses and 10 of 11 with UPJ masses were male. In contrast, the percentage of patients in the remainder of the cohort who were male was 68% (261 of 382). The median age of diagnosis for patients with PV masses, UPJ masses, and the IgG4-RD comparison group were 65.1, 65.4 and 61.8 years, respectively. Compared to all other IgG4-RD patients, those with PV masses had significantly higher median serum IgG4 values (891 vs 159 mg/dL, p=0.011) and median absolute and relative eosinophil counts (530 vs 180 cells/uL, p=0.015; 5.7 vs 2.7, p=0.015) (Table 1). IgG4-RD patients with PV masses were more likely to have lacrimal gland (71% vs 31%, p=0.036), submandibular gland (86% vs 41%, p=0.023), retroperitoneal (57% vs 17%, p=0.020), and lung involvement (57% vs 21%, p=0.042). In contrast, patients with UPJ masses were more likely to have prostate (40% vs 11%, p=0.02) and pericardial (18% vs 2%, p=0.028) involvement (Table 2).
Conclusion: Although masses in the PV and UPJ regions are considered highly suggestive of IgG4-RD, they occur in only a small minority of cases. Patients with either PV or UPJ masses tend overwhelmingly to be male, and those with PV masses have more exuberant immunologic disease activity (higher serum IgG4, more frequent peripheral eosinophilia) and more extensive organ involvement (higher frequency of lacrimal gland, submandibular gland, retroperitoneal, and lung involvement) compared to all other patients with IgG4-RD. In contrast, IgG4-RD patients presenting with UPJ masses are more likely to have prostate and pericardial involvement. Further studies incorporating imaging, histopathology, and treatment response among larger cohorts of IgG4-RD are needed to characterize these specific disease features further.
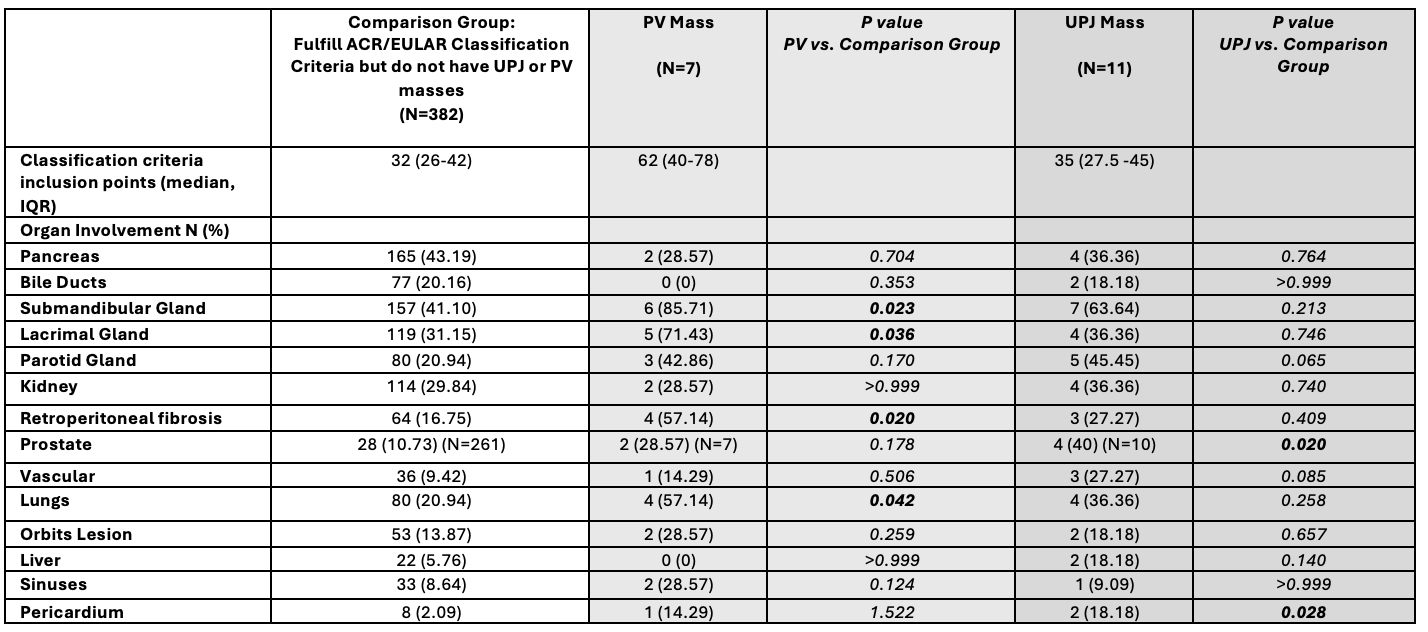 Table 1. Demographics and Laboratory Values for patients with paravertebral (PV) mass, ureteropelvic junction (UPJ) involvement, and remainder of the IgG4-RD cohort. P-values were calculated by comparing the UPJ and PV groups with the remainder of the cohort by applying Mann-Whitney U test for continuous variables, and Fisher’s exact test for categorical variables. Statistically significant p-values (p < 0.05) are shown in bold.
Table 1. Demographics and Laboratory Values for patients with paravertebral (PV) mass, ureteropelvic junction (UPJ) involvement, and remainder of the IgG4-RD cohort. P-values were calculated by comparing the UPJ and PV groups with the remainder of the cohort by applying Mann-Whitney U test for continuous variables, and Fisher’s exact test for categorical variables. Statistically significant p-values (p < 0.05) are shown in bold.
.jpg) Table 2. Organ Involvement distribution across the three groups. P-values were calculated by comparing the UPJ and PV groups with the remainder of the cohort by applying Fisher’s exact test. Statistically significant p-values (p < 0.05) are shown in bold.
Table 2. Organ Involvement distribution across the three groups. P-values were calculated by comparing the UPJ and PV groups with the remainder of the cohort by applying Fisher’s exact test. Statistically significant p-values (p < 0.05) are shown in bold.
.jpg) Figure 1. PV mass (A) and UPJ mass (B) imaging from two subjects of our cohort.
Figure 1. PV mass (A) and UPJ mass (B) imaging from two subjects of our cohort.
(A) Computed tomography (CT) scan showing 4.3 x 1.7 cm soft tissue mass spanning the visceral and paravertebral mediastinum at the T6-T8 level (orange arrow), from left to right axial and sagittal sections. (B) CT scan showing 2.6 cm ill-defined parapelvic soft tissue mass within the left kidney (yellow arrow).
To cite this abstract in AMA style:
Bonaso F, McMahon G, Jha I, Katz G, Wallace Z, Stone J, Perugino C. IgG4-Related Disease Paravertebral and Ureteropelvic Mass Presentations are Linked to Specific Disease Features [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/igg4-related-disease-paravertebral-and-ureteropelvic-mass-presentations-are-linked-to-specific-disease-features/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/igg4-related-disease-paravertebral-and-ureteropelvic-mass-presentations-are-linked-to-specific-disease-features/