Session Information
Date: Tuesday, October 28, 2025
Title: (2377–2436) Systemic Lupus Erythematosus – Diagnosis, Manifestations, & Outcomes Poster III
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Cardiovascular disease (CVD) is the most common cause of mortality among patients with systemic lupus erythematosus (SLE). Statin medications play a crucial role for the primary prevention of atherosclerotic cardiovascular disease (ASCVD), but data characterizing statin usage among patients with SLE are scarce. We sought to identify patterns of statin use for primary prevention of ASCVD in patients with SLE.
Methods: We identified an SLE cohort from TriNetX, an electronic health record (EHR) database with patients from academic, community, and private medical centers across the United States. We included patients with SLE (≥2 ICD codes ≥30 days and ≤2 years apart) between January 2000 and August 2021. We utilized the 2018 American Heart Association Guideline on the Management of Blood Cholesterol and the Pooled Cohort Equation (PCE) to identify SLE patients with an indication for treatment with a moderate or high intensity statin for primary prevention of ASCVD (indications include a 10-year risk of ASCVD ≥7.5%, diabetes, or LDL ≥190 mg/dL. We also performed a variation of ASCVD risk estimation by doubling the risk calculated by the PCE (modified PCE) to account for increased risk conferred by SLE. We assessed statin use patterns among eligible patients and examined factors associated with underutilization using multivariable logistic regression, adjusting for 10-year ASCVD risk.
Results: There were 21,926 SLE patients between ages 40-75 without prior ASCVD who underwent at least one ASCVD risk assessment with cholesterol and blood pressure monitoring (Figure 1). After excluding 355 patients with contraindications to statin therapy (i.e., pregnancy and liver failure), 9,456 patients (43.8%) had an indication for a moderate or high-intensity statin. Of these, 5,039 (53.3%) received a statin. Among the 3216 patients with a PCE risk score ≥20% or LDL ≥190 mg/dL, 1303 (40.5%) never received a statin. Employing the modified PCE, an additional 2827 patients (13.1%) were eligible for a moderate or high-intensity statin, of whom 871 (30.8%) received a statin in primary prevention. Among those with an indication, Black individuals (adjusted OR [aOR] 1.40 [95% CI 1.27-1.54]) and patients below the age of 60 (aOR 2.09 [95% CI 1.90-2.30]) were more likely to receive a moderate or high-intensity statin, as were those with comorbidities such as diabetes (aOR 1.91 [95% CI 1.76-2.08]), hypertension (aOR 1.16 [95% CI 1.07-1.26]) and hyperlipidemia (aOR 1.91 [95% CI 1.75-2.08], Table 1). There was no difference in statin use in the subset of patients with lupus nephritis (aOR 0.95 [95% CI 0.84-1.09]).
Conclusion: In this large EHR-based cohort of patients with SLE, 44% met criteria for a moderate or high-intensity statin for primary prevention of ASCVD, but only around half of eligible patients received a statin. These findings highlight the significant underutilization of statin therapy among patients with SLE, a population of individuals with enhanced risk for CVD.
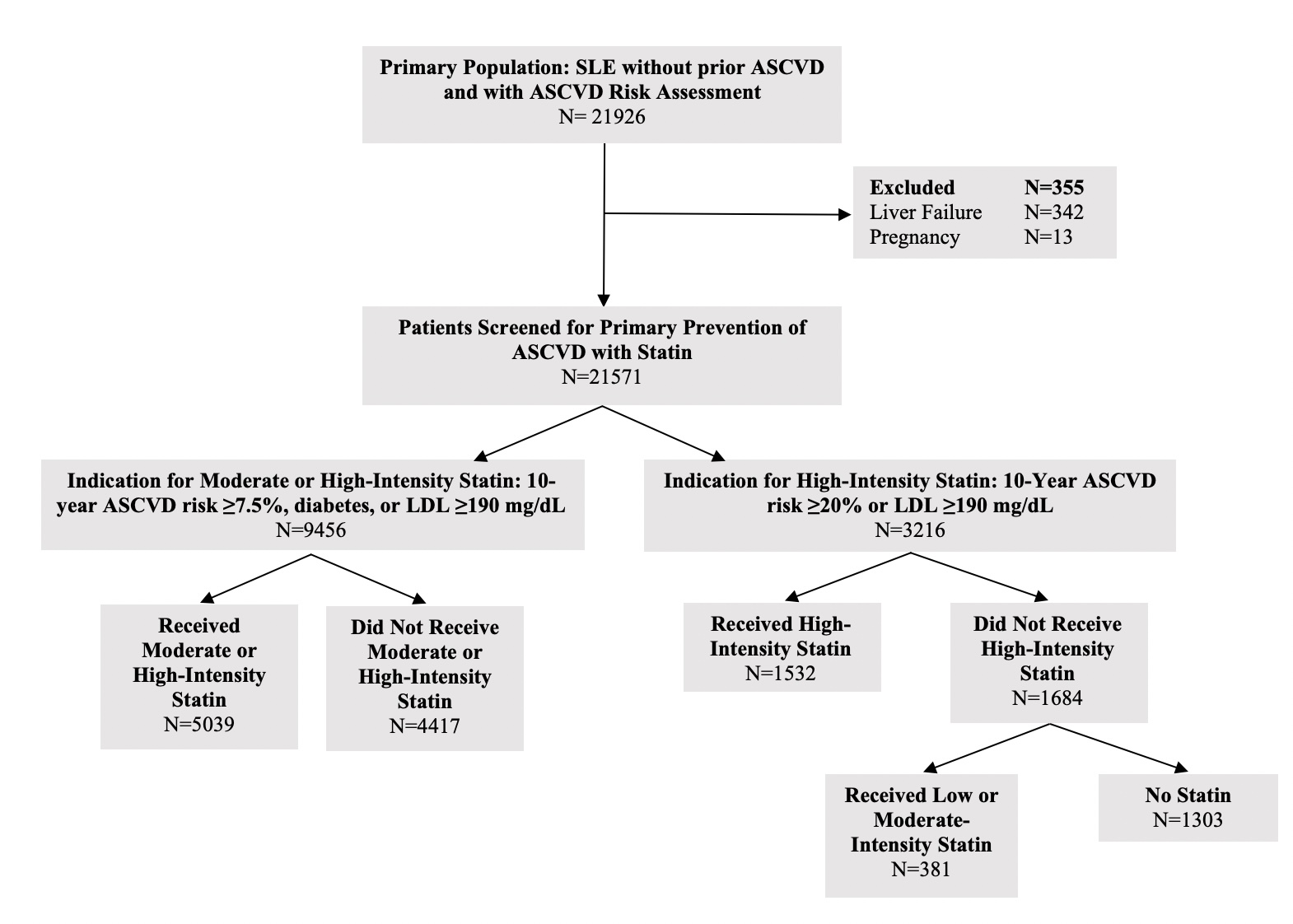 Figure 1: Assessment of Statin Use in Patients with Systemic Lupus Erythematosus for the Primary Prevention of Atherosclerotic Cardiovascular Disease (ASCVD) According to the 2018 American Heart Association Guideline on the Management of Blood Cholesterol
Figure 1: Assessment of Statin Use in Patients with Systemic Lupus Erythematosus for the Primary Prevention of Atherosclerotic Cardiovascular Disease (ASCVD) According to the 2018 American Heart Association Guideline on the Management of Blood Cholesterol
.jpg) Table 1: Factors Associated with Moderate or High-Intensity Statin Use Among Patients with Systemic Lupus Erythematosus with an Indication for Primary Prevention of Atherosclerotic Cardiovascular Disease
Table 1: Factors Associated with Moderate or High-Intensity Statin Use Among Patients with Systemic Lupus Erythematosus with an Indication for Primary Prevention of Atherosclerotic Cardiovascular Disease
To cite this abstract in AMA style:
Patel A, Zhang L, Lau E, Choi H, Jorge A. Statin Use for Primary Prevention of Atherosclerotic Cardiovascular Disease Among Patients with Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/statin-use-for-primary-prevention-of-atherosclerotic-cardiovascular-disease-among-patients-with-systemic-lupus-erythematosus/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/statin-use-for-primary-prevention-of-atherosclerotic-cardiovascular-disease-among-patients-with-systemic-lupus-erythematosus/