Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Interstitial lung disease (ILD) is a severe extra-articular manifestation of rheumatoid arthritis (RA). Abatacept (ABA) has demonstrated effectiveness in the treatment of RA-ILD, regardless radiological pattern. Although global results are satisfactory, there are patients who present progression of ILD. The early identification of this group of patients is crucial for a prompt and adequate treatment. In a wide series of RA-ILD treated with ABA, our aim was to characterize the subgroup of patients with progressive RA-ILD.
Methods: From a large observational multicenter study of 526 RA-ILD patients treated with ABA, we selected those with available pulmonary function tests (PFTs) at baseline and in follow-up. Progressive ILD was defined as an absolute decline of forced vital capacity (FVC) of ≥10% within 2 years of follow-up since ABA initiation. Results are expressed as percentage, mean±SD or median [IQR] as appropriate. A comparative study and multivariable analysis of patients with progressive ILD and the remaining patients was performed.
Results: We finally included a total of 343 patients with available data on FVC of which 80 (23.3%) presented progressive ILD and 263 (76.7%) had a favorable lung function course (Figure). The differential baseline general characteristics between both groups are displayed in Table 1. We found no statistically differences in age, sex, smoking, ILD duration up to ABA initiation, positivity of rheumatoid factor or anti-citrullinated protein autoantibodies, combined treatment, prednisone dose, baseline PFTs or radiological pattern. Patients with progressive-ILD had a statistically higher dyspnea score and a lower proportion of patients had received previously methotrexate (63% vs 76%, p=0.02) and tocilizumab (5% vs 13%, p=0.048). Multivariable analysis (Table 2) showed that previous treatment with methotrexate or golimumab or joint activity (measured by DAS28ESR) multiplies by 0.453, 10.009 or 1.284, respectively, the probability of progressive ILD.
Conclusion: Almost a quarter of patients with ABA therapy presented progressive ILD. The main general features at ABA initiation are very similar in progressive and non-progressive ILD groups. Previous treatment with methotrexate seems to be a protective factor for ILD progression. Although ABA has consistently demonstrated effectiveness in the treatment of RA-ILD, its response, including joint inflammation, should be closely monitored.
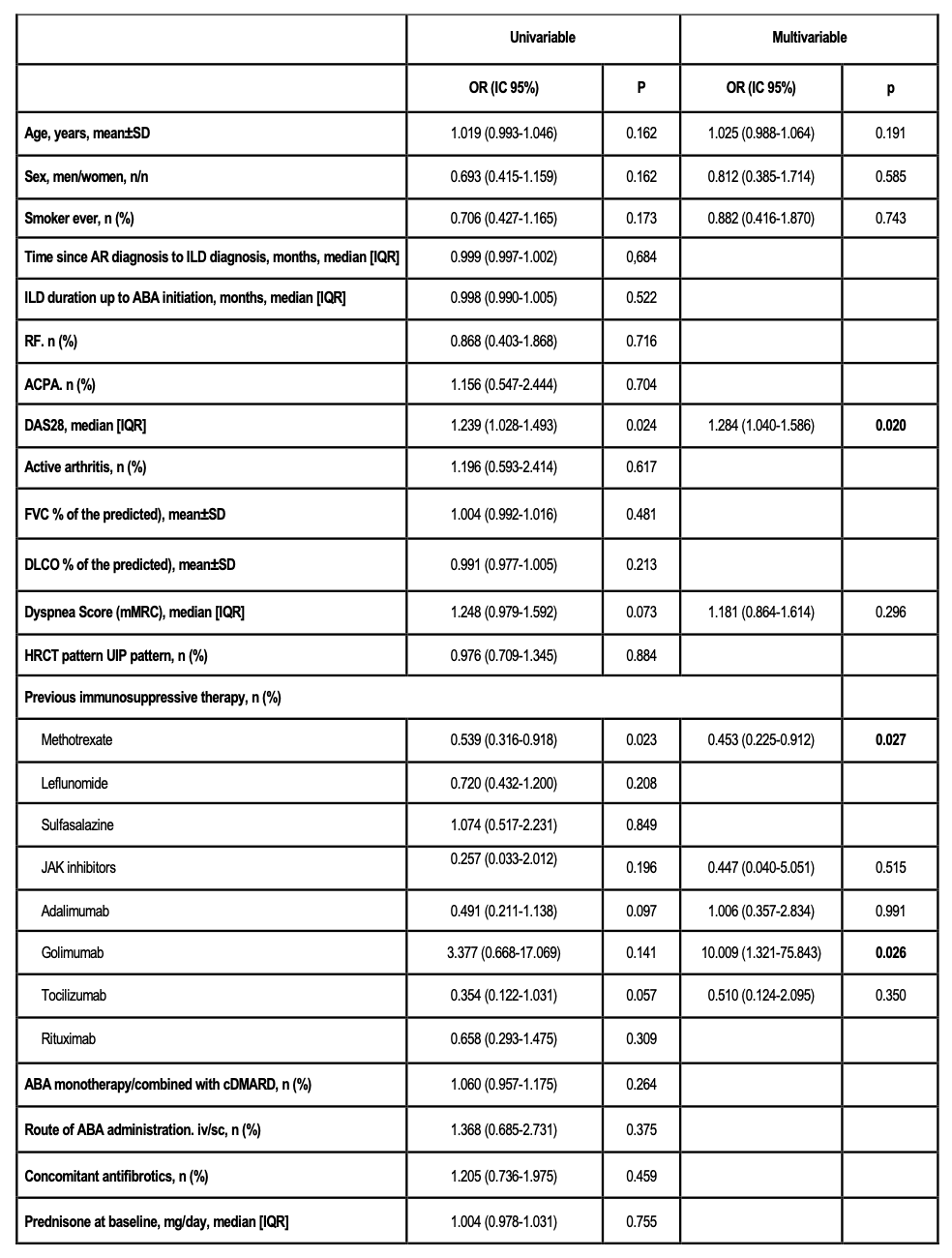 Table 1. Comparison of main baseline (abatacept initiation) features of RA-ILD patients treated with ABA divided into progressive ILD and non-progressive groups.
Table 1. Comparison of main baseline (abatacept initiation) features of RA-ILD patients treated with ABA divided into progressive ILD and non-progressive groups.
.jpg) Table 2. Multivariable analysis through logistic regression of associative factors of ILD progression at 24 months.
Table 2. Multivariable analysis through logistic regression of associative factors of ILD progression at 24 months.
.jpg) Figure. Evolution of FVC in patients included in “ILD progression” group vs in those included in “non ILD progression” (progression of ILD was defined as an absolute decline of forced vital capacity (FVC) of ≥10% within 2 years of follow-up since ABA initiation). * p < 0.05.
Figure. Evolution of FVC in patients included in “ILD progression” group vs in those included in “non ILD progression” (progression of ILD was defined as an absolute decline of forced vital capacity (FVC) of ≥10% within 2 years of follow-up since ABA initiation). * p < 0.05.
To cite this abstract in AMA style:
Serrano-Combarro A, Atienza-mateo B, Martin-Gutierrez A, López-Maraver M, Ibarrola L, Casafont-Solé I, Loarce J, Blanco-Madrigal J, Castañeda S, Ortega-Castro R, Mena Vázquez N, Vegas Revenga N, Domínguez-Casas L, Peralta-Ginés C, Fernández Díaz C, Loricera J, Blanco R. Progressive Interstitial Lung Disease associated to Rheumatoid Arthritis despite Abatacept therapy. Data from a large national multicenter cohort of 526 patients [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/progressive-interstitial-lung-disease-associated-to-rheumatoid-arthritis-despite-abatacept-therapy-data-from-a-large-national-multicenter-cohort-of-526-patients/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/progressive-interstitial-lung-disease-associated-to-rheumatoid-arthritis-despite-abatacept-therapy-data-from-a-large-national-multicenter-cohort-of-526-patients/