Session Information
Date: Tuesday, October 28, 2025
Title: (2227–2264) Rheumatoid Arthritis – Diagnosis, Manifestations, and Outcomes Poster III
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Interstitial lung disease (ILD) in Rheumatoid Arthritis (RA) determines a worse prognosis with an increased mortality. Abatacept and rituximab may be the preferred therapies. JAK inhibitors (JAKi) have demonstrated effectiveness in observational studies of RA-ILD, especially with tofacitinib or baricitinib (BARI). While both articular and pulmonary domains may respond to JAKi, some patients experience ILD progression. Identifying this subgroup of patients is essential for early detection and appropriate management. In a large series of RA-ILD patients treated with BARI, we aimed to a) study the effectiveness, and b) characterize the subgroup with progressive ILD.
Methods: From a large observational multicenter study of 72 RA-ILD patients treated with BARI, we selected those with available pulmonary function tests (PFTs) follow-up data. Progressive ILD was defined as an absolute decline of forced vital capacity (FVC) of ≥10% within 1 year of follow-up since BARI initiation (Figure). We compared patients with and without progressive ILD. Results are expressed as percentage, mean±SD or median [IQR], as appropriate.
Results: A total of 42 patients with available data on FVC evolution were included. Progressive and non-progressive ILD was observed in 11 (26%) and 31 (74%) patients, respectively. The baseline general features are summarized in Table. Both groups were similar in age, smoking, positivity of rheumatoid factor or anti-citrullinated protein autoantibodies, ILD duration up to BARI initiation, prednisone dose, baseline PFTs or radiological pattern. Progressive ILD was more frequent in women and as expected required more combined treatment with antifibrotics. FVC evolution in both groups (progressive and non-progressive ILD) and by sex is displayed in figure.
Conclusion: BARI may be useful in RA-ILD. However, progression may be present in around a quarter of patients, especially in women. Effectiveness should be closely monitored with PFTs to early detect progressive ILD.
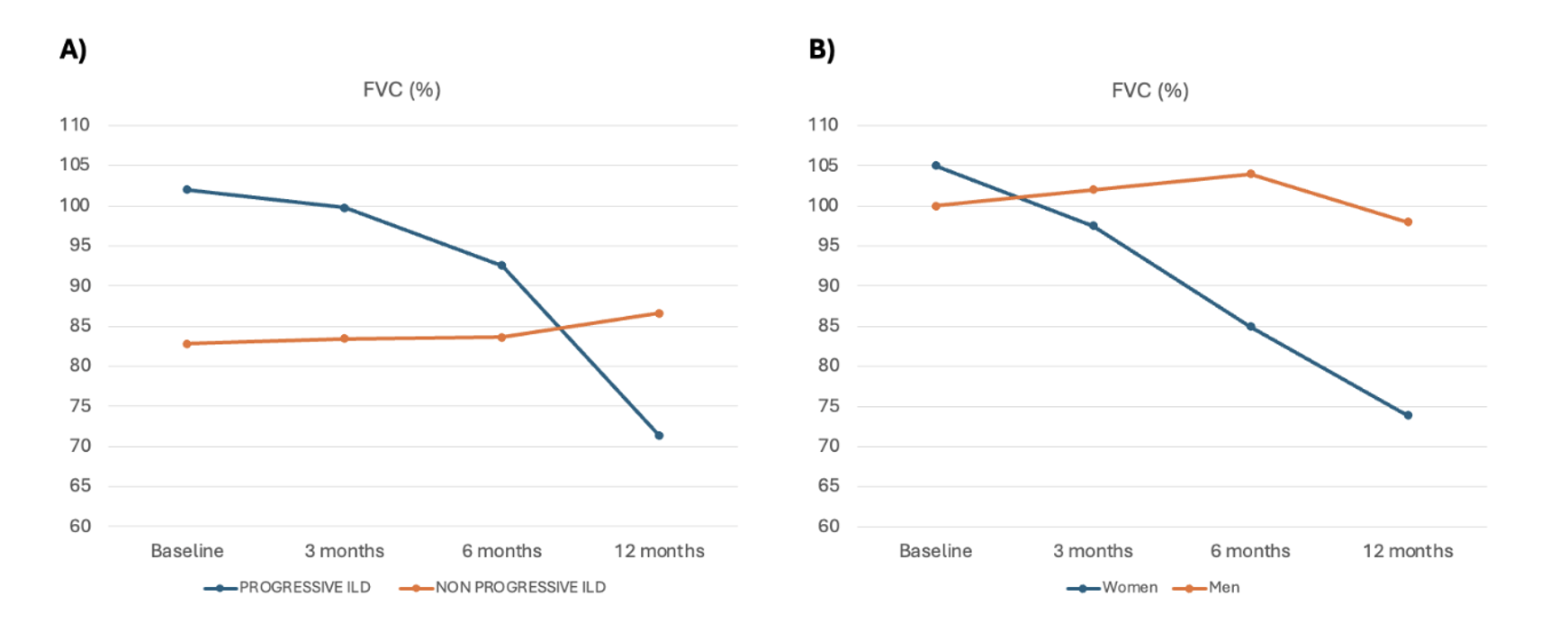 Table. Baseline characteristics of RA-ILD patients treated with BARI.
Table. Baseline characteristics of RA-ILD patients treated with BARI.
.jpg) Figure. FVC evolution in A) both groups (progressive and non-progressive ILD) and B) by sex. Progressive ILD was defined as an absolute decline of forced vital capacity (FVC) of ≥10% within 1 year of follow-up since BARI initiation).
Figure. FVC evolution in A) both groups (progressive and non-progressive ILD) and B) by sex. Progressive ILD was defined as an absolute decline of forced vital capacity (FVC) of ≥10% within 1 year of follow-up since BARI initiation).
To cite this abstract in AMA style:
Serrano-Combarro A, Atienza-mateo B, Loarce J, Egües Dubuc C, Pastor Mena M, Melero-González R, Rojas Herrera S, Carrasco-Cubero C, Perez Garcia C, Blanco-Madrigal J, Vegas Revenga N, Palma-Sanchez D, García-Valle A, Ruiz-Esquide V, Lamua-Riazuelo J, Castañeda S, Blanco R. National Multicenter study of Baricitinib in Rheumatoid Arthritis – Interstitial Lung Disease: effectiveness and progressive lung disease [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/national-multicenter-study-of-baricitinib-in-rheumatoid-arthritis-interstitial-lung-disease-effectiveness-and-progressive-lung-disease/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/national-multicenter-study-of-baricitinib-in-rheumatoid-arthritis-interstitial-lung-disease-effectiveness-and-progressive-lung-disease/