Session Information
Date: Tuesday, October 28, 2025
Title: (1972–1989) Measures & Measurement of Healthcare Quality Poster II
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: In 2017, FDA approved warnings regarding fatal cardiac effects such as cardiomyopathy, torsades de pointes, and QTc prolongation related to both acute and chronic Hydroxychloroquine (HCQ) use. QTc >470 ms during HCQ treatment was associated with increased mortality risk1. COVID-19 pandemic in 2020 reemerged discussions regarding HCQ’s cardiotoxicity as it was experimentally used in the acute setting. In 2021, a white paper on consensus between rheumatologists and cardiologists was released by ACR2. While it acknowledged that the foundational benefits of HCQ outweigh the associated cardiac risks in SARD patients, it mentioned utilizing ECG for patients with high-risk cardiovascular (CV) factors. These factors include female, older age ( >68 years), recent heart disease, prolonged duration of HCQ use, and >1 QTc-prolonging medications, such as concurrent fibromyalgia and depression/anxiety, prevalent in the SARD population. Hence, this study aims to increase cardiac screening/monitoring through routine ECG, particularly in SARD patients with high CV risks on HCQ.
Methods: This quality improvement (QI) project retrospectively analyzed medical records of patients at least 18 years old on HCQ seen at University of Florida rheumatology clinic sites from 06/2023 to 12/2023 and had ECG done within the past year as initial data (pre-intervention phase). Coordination with cardiology and scheduling team allowed same-day walk-in ECG, especially for high-risk patients based on cardiac risk stratification, increasing ECG accessibility. Interventions also included creating flyers and educating medical staff periodically. Documentation of ECG results was facilitated by generating smart phrases into patient’s visit note under the specific cardiac risk stratification and diagnosis. Subsequent retrospective chart review of 50 patients was performed after 12 months to analyze impact of interventions.
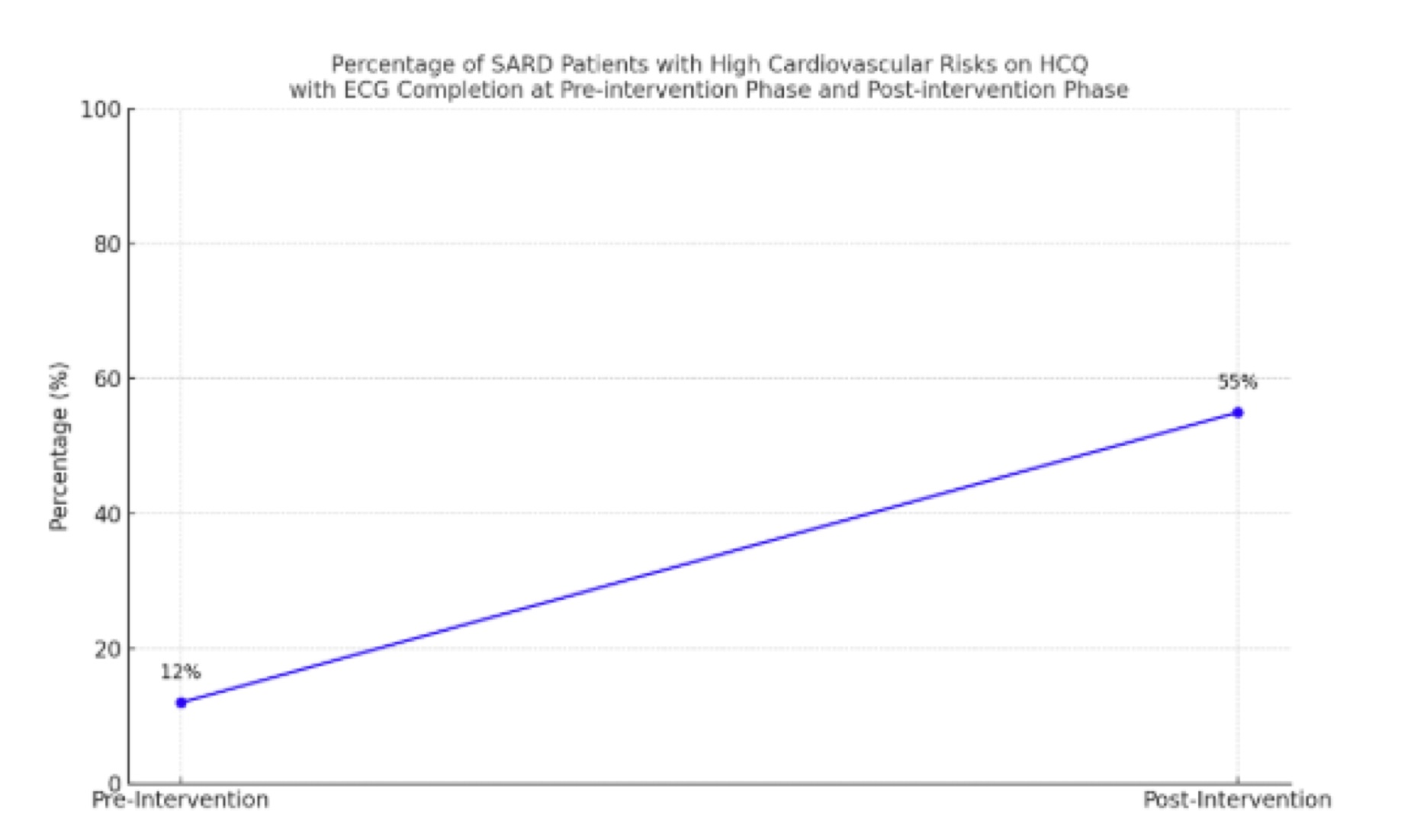
Results: Initial data showed the need for increasing ECG testing in our high-risk SARD patients (Table 1). All patients were on adequate HCQ dosing. Only 12% had baseline ECG within past year. Post-intervention, this percentage increased to 55%, with more than 2/3 done on same-day rheumatology visits along with electronic documentation of ECG and cardiac risk stratification. Eight percent had QTc 470–500 ms; 3 patients with QTc >500 ms were associated with more acute settings (ESRD, acute admission, and pacemaker) (Figures 1 and 2). Risks vs benefits discussions and decisions on adjusting HCQ dose based on weight and HCQ levels, closer monitoring, and even switching to another DMARD were done accordingly.
Conclusion: This QI project demonstrates routine ECG as simple and inexpensive cardiac screening/monitoring tool for SARD patients with high CV risks on HCQ. We developed interventions (interdepartment collaboration, etc) that facilitated ECG accessibility, identification of cardiac risk stratification, improved documentation and modification, and monitoring of current treatment regimen based on their CV risk factors and disease activity. This study answers ACR’s call for addressing the ongoing need for evaluating HCQ’s rare but fatal cardiotoxic risks among our SARD patients with high CV risks on HCQ.
.jpg)
.jpg) Figure 2. Percentage of SARD patients with High Cardiovascular Risks on HCQ with ECG Completion at the Pre-intervention Phase and Post-intervention Phase.
Figure 2. Percentage of SARD patients with High Cardiovascular Risks on HCQ with ECG Completion at the Pre-intervention Phase and Post-intervention Phase.
To cite this abstract in AMA style:
Kuzhuppilly Arcilla C, Kirsch G, Kaeley G, Thway M. Baseline QTc Screening and Monitoring Among SARD Patients with High Cardiovascular Risks on Hydroxychloroquine Based on 2021 ACR Consensus: A Quality Improvement Project [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/baseline-qtc-screening-and-monitoring-among-sard-patients-with-high-cardiovascular-risks-on-hydroxychloroquine-based-on-2021-acr-consensus-a-quality-improvement-project/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/baseline-qtc-screening-and-monitoring-among-sard-patients-with-high-cardiovascular-risks-on-hydroxychloroquine-based-on-2021-acr-consensus-a-quality-improvement-project/