Session Information
Date: Monday, October 27, 2025
Title: (1467–1516) Systemic Lupus Erythematosus – Diagnosis, Manifestations, & Outcomes Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: LLDAS is a desirable state in lupus, with ongoing global reports on its durability and outcomes. The relationship between LLDAS, baseline characteristics, and drug efficacy is unknown. A university hospital’s SLE registry (since 1998) describes the frequency, duration, and outcomes after achieving LLDAS in patients followed for ≥5 years.
Methods: Patients fulfilling the updated 1997 ACR or 2012 SLICC criteria with at least one follow-up clinic visit annually for a minimum of five years, were included. The registry records baseline disease characteristics, SLEDAI score, SLICC/ACR Damage Index, serologies, and treatment in each clinic visit and is approved by the Institutional Ethics Committee. Records with missing data on clinical SLEDAI in more than 3 contiguous visits or deaths/ lost followup within 5 years and when the disease course could not be inferred by registry notes were excluded. HDAS before LLDAS was defined by either 1 BILAG A, 2 BILAG B, or clinical SLEDAI >6. LLDAS was scored if all five predefined criteria (Franklyn K et al) were fulfilled. LLDAS50 was recorded if at least half of the observation period was spent in LLDAS.The study used non-parametric descriptive statistics for summarizing non-normally distributed data and generalized estimating equations (GEE) to identify predictors of LLDAS50. Group comparisons were performed using Mann-Whitney U tests and Chi-square tests as appropriate.Aim – To characterize the attainment and maintenance of LLDAS over time in a cohort of SLE ObjectivesTo determine frequency, predictor and time to flare following LLDASTo identify the frequency and predictors of LLDAS50
Results: This study included a cohort of 307 (282 females) patients (Table 1) with 2679.6 patient-years of observation, averaging 3.15 ± 3.4 observations per patient per year. A large proportion (266 of 307, 86%) exhibited HDAS before achieving their first LLDAS. During the observation period 291 (94.7%) achieved LLDAS, 142 maintained it till last visit while 228 (78%) attained LLDAS50. Flares occurred in 154 patients (severe in 111). Median (IQR) time to flare was 2.89 (1.48, 4.95) years. Most (45%) flares occurred within 2 years of first attaining LLDAS. Differences in LLDAS characteristics in patients with and without prior HDAS is presented in Table 2. GEE models showed that patients with hematologic or musculoskeletal involvement (OR and p value 0.48, 0.011; 0.39, 0.04 respectively) or cyclophosphamide use (OR 0.41, p 0.01) did not attain LLDAS50 (Figure 1). At their last recorded visit, 194/291 (66%) patients were in LLDAS with one-third (102 of 307) off glucocorticoids. SDI was 0 in 43.4%, with some damage present in the others. Limitations: This study does not include patients who died or were lost to follow-up within five years of first being seen at the hospital. Periods of non-compliance are not reliably captured.
Conclusion: In patients attending lupus clinic for more than five years, LLDAS is achieved by most early active lupus survivors but not often sustained. Patients with hematological and musculoskeletal involvement are less likely to achieve LLDAS50. High initial disease activity is associated with reduced time in LLDAS, earlier, more severe flares and flares after steroid/IS taper.
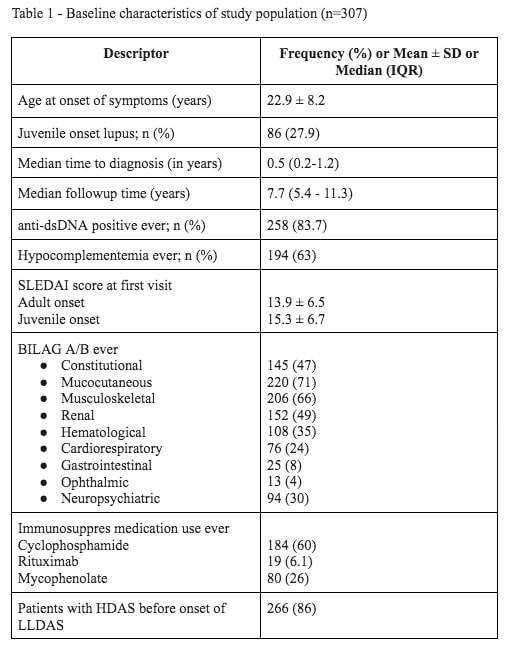 Table 1 – Baseline characteristics of study population (n=307)
Table 1 – Baseline characteristics of study population (n=307)
.jpg) Table 2: Characteristics of LLDAS achiever’s (n=291) stratified by prior High Disease Activity Status (HDAS)
Table 2: Characteristics of LLDAS achiever’s (n=291) stratified by prior High Disease Activity Status (HDAS)
.jpg) Figure 1: Predictors of LLDAS50
Figure 1: Predictors of LLDAS50
To cite this abstract in AMA style:
Gopalan A, yerram k, Gaikwad M, rajasekhar L. Characteristics and Predictors of LLDAS in Survivors of Early Active Lupus: Insights from a Decade-Long Cohort [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/characteristics-and-predictors-of-lldas-in-survivors-of-early-active-lupus-insights-from-a-decade-long-cohort/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/characteristics-and-predictors-of-lldas-in-survivors-of-early-active-lupus-insights-from-a-decade-long-cohort/