Session Information
Date: Monday, October 27, 2025
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Ankylosing spondylitis (AS) is a chronic inflammatory disease with systemic complications that may contribute to increased mortality risk. This study examines the characteristics and causes of in-hospital death among adult AS patients in the United States using a claims-based database.
Methods: A retrospective analysis of all adult hospitalizations with a diagnosis of AS (ICD-10: M45) in the National Inpatient Sample (NIS) database (2017 – 2021) was conducted. Descriptive statistics were used to analyze demographics, hospital length of stay (LOS), insurance status, total hospital charges, and causes of death categorized by ICD-10 codes.
Results: Of the 96,330 adult AS hospitalizations in the 2017 – 2021 NIS database, 2,390 (2.5%) died in the hospital (Table 1). AS patients who died compared to those discharged alive were more likely to be male (79.7% vs. 62.9%; p < 0.001), were older (median age 73 vs. 62 years; p < 0.001), had longer median hospital LOS (7 vs. 4 days; p < 0.001), had higher median total hospital charges ($104,275 vs. $44,345; p < 0.001), more Medicare (73.6% vs. 54.6%; p < 0.001), less Medicaid (4.8% vs. 10.3%; p < 0.001), less private insurance (16.3% vs. 30.1%; p < 0.001), and a lower percentage of the top household income quartile (18.6% vs. 24.9%; p = 0.002). Racial distribution did not significantly differ between groups.The causes of in-hospital death of AS patients as determined by their “principal ICD-10 billing diagnosis category” were as follows: injury/poisoning (29.1%), infections (22.0%), cardiovascular (CV) diseases (11.3%), respiratory diseases (11.1%), hematologic/oncologic conditions (7.5%), gastrointestinal diseases (5.0%), genitourinary diseases (3.1%), factors influencing health status (1.5%), rheumatologic diseases (1.3%), neurologic diseases (0.8%), endocrine diseases (0.6%), and other causes (0.6%) (Table 2).The most common specific injury diagnosis was traumatic subdural hemorrhage (ICD-10: S06.5X0A) (table 3), followed by fractures of the thoracic (ICD-10: S22.089A, S22.088A, S22.078A, S22.069A, S22.079A), cervical (ICD-10: S12.300A, S12.400A, S12.490A, S12.200A), and lumbar vertebrae (ICD-10: S32.019A). Severe spinal cord injuries (ICD-10: S14.115A, S24.102A, S24.103A, S14.106A), traumatic subarachnoid hemorrhage (ICD-10: S06.6X0A), and thoracic trauma, including hemothorax and hemopneumothorax (ICD-10: S27.1XXA, S27.2XXA), were also frequent (Table 3).
Conclusion: Our analysis represents the only report to date to comprehensively study AS inpatients on a U.S. national level. Over 1 of 50 AS hospitalizations ended in death, and they were predominantly older males, most of whom had Medicare insurance. Injury-related conditions were the most frequent cause of death. The leading injury diagnoses were brain bleeds, vertebral fractures, and spinal cord injuries. Further research is needed to explore the factors contributing to injuries and falls in AS patients.
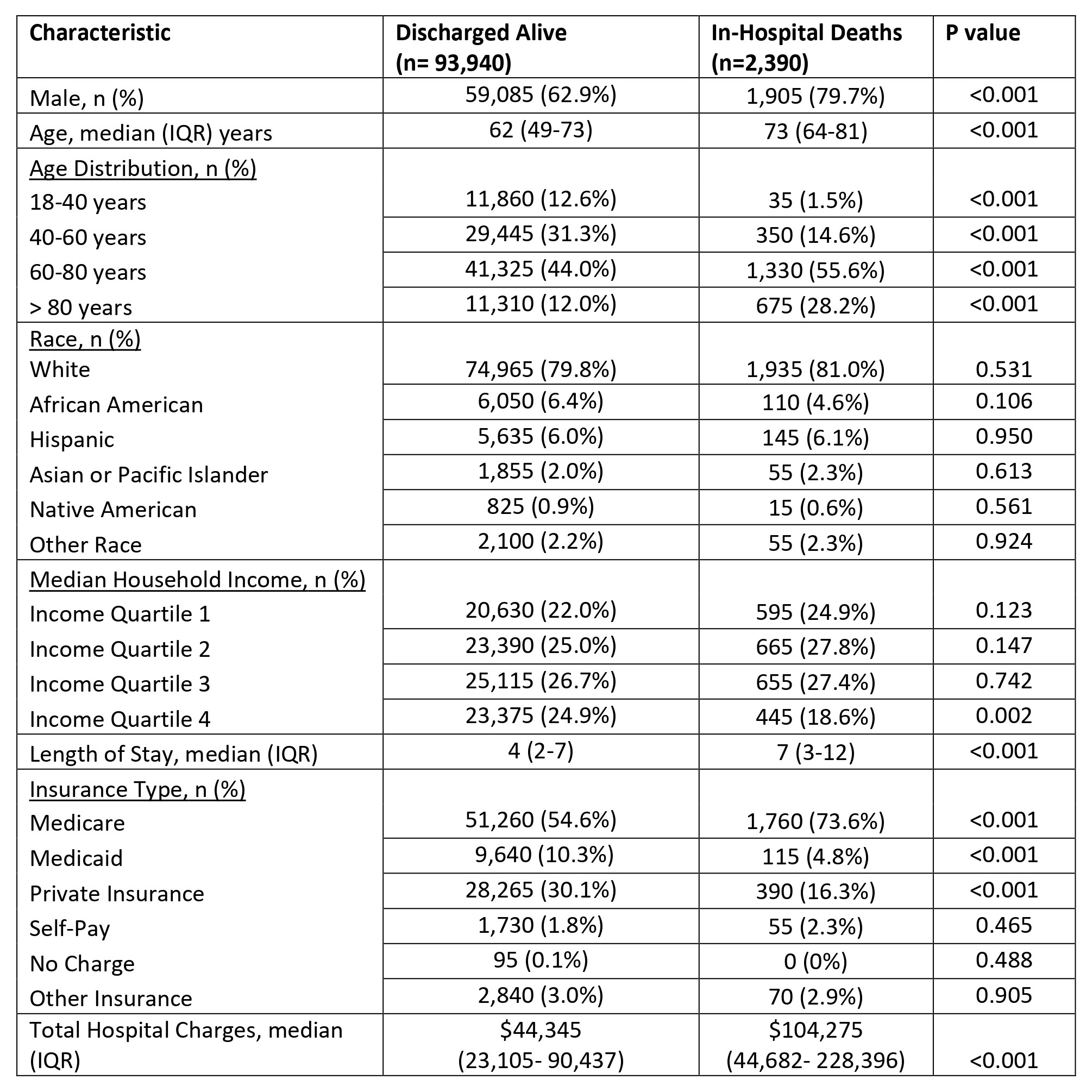 Table 1. Descriptive Characteristics of Adult Ankylosing Spondylitis Patients from 2017 – 2021 National Inpatient Sample Database (n = 96,330).
Table 1. Descriptive Characteristics of Adult Ankylosing Spondylitis Patients from 2017 – 2021 National Inpatient Sample Database (n = 96,330).
Abbreviations: AS = ankylosing spondylitis; n = number; IQR = interquartile range
.jpg) Table 2. Causes for In-Hospital Death of Adult Ankylosing Spondylitis Patients from the National Inpatient Sample Database 2017 – 2021 (n = 2,390).
Table 2. Causes for In-Hospital Death of Adult Ankylosing Spondylitis Patients from the National Inpatient Sample Database 2017 – 2021 (n = 2,390).
Abbreviations: AS = ankylosing spondylitis; n = number; NR = not reported as below permitted reporting threshold rules for National Inpatient Sample
.jpg) Table 3: Top Injury Causes of In-Hospital Death in Adult AS patients from National Inpatient Sample Database.
Table 3: Top Injury Causes of In-Hospital Death in Adult AS patients from National Inpatient Sample Database.
To cite this abstract in AMA style:
Small I, Natu A, Manadan A. A Nationwide Analysis of In-Hospital Mortality in Adult Ankylosing Spondylitis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/a-nationwide-analysis-of-in-hospital-mortality-in-adult-ankylosing-spondylitis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-nationwide-analysis-of-in-hospital-mortality-in-adult-ankylosing-spondylitis/