Session Information
Date: Monday, October 27, 2025
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Primary Sjӧgren’s syndrome is a multisystem autoimmune disorder characterized by progressive dysfunction of exocrine glands leading to symptoms of keratoconjunctivitis and xerostomia. There is no cure for Sjӧgren’s syndrome, however a multidisciplinary approach with care from a rheumatologist, dentist, and ophthalmologist can be adopted to help manage symptoms. Diagnosis of the condition can be difficult due to the overlap between Sjӧgren’s syndrome and other diseases. In 2016 the ACR-EULAR classification criteria for primary Sjӧgren’s syndrome were established. Application of these classification criteria, especially for enrollment in clinical trials, can help differentiate between primary Sjӧgren’s syndrome and patients that need further evaluation.. Accurate classification of patients is crucial for their treatment and prognosis.
Methods: We analyzed a quaternary medical center-based biobank cohort identifying patients with 2+ ICD codes associated with Sjӧgren’s syndrome. This was done as a subset of a study investigating patients with interstitial lung disease (ILD) within the biobank, Patients also had 2+ codes associated with ILD as well as 1+ codes for computed tomography scan of the chest. Patient records were manually reviewed for information leading to a definitive, probable, possible, or unlikely classification of primary Sjӧgren’s syndrome using the 2016 ACR-EULAR classification criteria (Table 1). Patient characteristics were compared using Kruskal-Wallis and chi-square tests. We calculated positive predictive value (PPV) for each of the ICD codes associated with Sjӧgren’s syndrome to assess whether code-based algorithms could be used to predict definitive Sjӧgren’s syndrome.
Results: Eighty-three patients with codes of interest were identified within the biobank cohort (Table 2). Of these 83 patients, 14 (17%) fit classification criteria for definitive Sjӧgren’s syndrome, 23 (28%) – for probable Sjӧgren’s syndrome, 20 (24%) -for possible Sjӧgren’s syndrome, and 26 (31%) were unlikely to be classified with primary Sjӧgren’s syndrome. Positive anti-SSA (Ro) was the most common classification criteria seen among the 71 (86%) patients who underwent serological testing in the cohort. Diagnosis of Sjӧgren’s syndrome by a rheumatologist was noted in 55% of the total cohort but in 100% of the definitive subgroup. None of the ICD codes had a high PPV for definitive Sjӧgren’s syndrome category by chart review (Table 3).
Conclusion: This work highlights the difficulty with the classification of Sjögren’s syndrome even within a group of patients that have multiple diagnostic codes for the condition. A large proportion of patients had missing data, many did not have serological or clinical testing available for review. Continued education for providers who are likely to evaluate patients for Sjögren’s syndrome in their clinic, such as primary care or ophthalmology, is crucial to improve diagnosis and patient care. Future directions include development of an algorithm to help accurately classify patients with definitive Sjögren’s syndrome without extensive chart review.
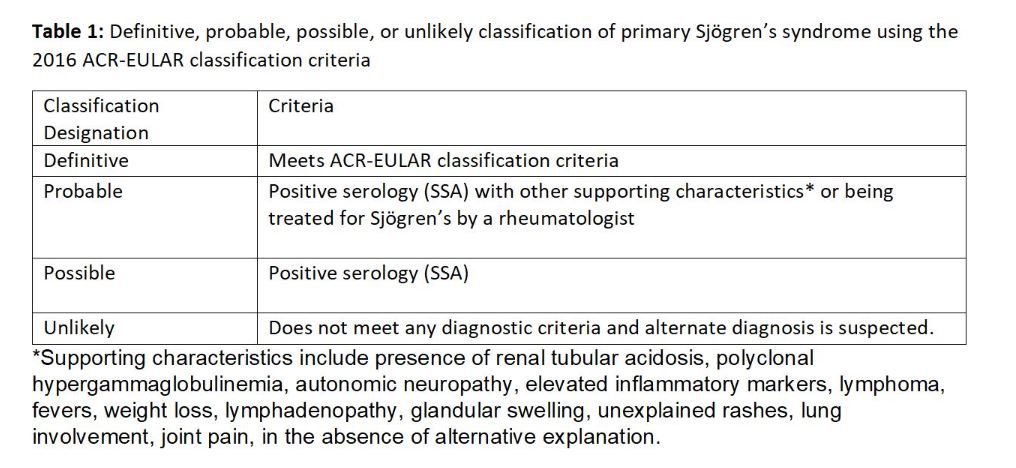 Table 1: Definitive, probable, possible, or unlikely classification of primary Sjӧgren’s syndrome using the 2016 ACR-EULAR classification criteria
Table 1: Definitive, probable, possible, or unlikely classification of primary Sjӧgren’s syndrome using the 2016 ACR-EULAR classification criteria
.jpg) Table 2: Characteristics of patients with 2+ diagnostic codes for Sjӧgren’s syndrome
Table 2: Characteristics of patients with 2+ diagnostic codes for Sjӧgren’s syndrome
.jpg) Table 3: PPV of various ICD codes in predicting definitive Sjӧgren’s syndrome classification subtypes
Table 3: PPV of various ICD codes in predicting definitive Sjӧgren’s syndrome classification subtypes
To cite this abstract in AMA style:
Clement K, Crowson C, Achenbach s, myasoedova E, carmona e, Vassallo R, Kronzer V, Joerns e. Positive predictive value of various diagnostic codes for the classification of primary Sjӧgren’s syndrome [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/positive-predictive-value-of-various-diagnostic-codes-for-the-classification-of-primary-sj%d3%a7grens-syndrome/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/positive-predictive-value-of-various-diagnostic-codes-for-the-classification-of-primary-sj%d3%a7grens-syndrome/