Session Information
Date: Monday, October 27, 2025
Title: (1306–1346) Rheumatoid Arthritis – Diagnosis, Manifestations, and Outcomes Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Interstitial lung disease (ILD) is a frequent and severe complication of rheumatoid arthritis (RA). Although early diagnosis and screening of ILD in RA patients with risk factors is recommended, there is no current consensus on how to perform screening of ILD in these patients. Spanish guidelines (SER-SEPAR screening criteria) recommend chest x-ray (CXR) and pulmonary function test (PFT) to patients with dyspnoea or cough > 3 months and asymptomatic patients with an intermediate risk for ILD. Portuguese guidelines recommend CXR and PFT as screening in patients without symptoms or risk factors for ILD. ACR/CHEST guidelines conditionally recommend against screening with CXR but considers screening with PFT.The aim of this study is to assess the diagnostic yield of CXR and PFT for diagnosing ILD in patients with RA.
Methods: This is a retrospective study that included patients with RA fulfilling ACR/EULAR 2010 classification criteria that had a thoracic computerized tomography (CT) between 01/01/2020 and 31/12/2024. ILD was diagnosed according to the CT results. CXR and PFT (spirometry and diffusing capacity of lung for carbon monoxide [DLCO]) performed a maximum of 12 months previous to the CT were reviewed. CXR were interpreted blindly to the patient clinical data and classified as normal or abnormal (which included findings suggestive of ILD or another lung pathology that would require a CT). Sensitivity and specificity were calculated for each item individually and combined for diagnosing ILD, using CT as the gold standard. We compared patients with ILD and without ILD using χ2 (with Fisher correction as appropriate) for categorical variables and t test/Mann-Whitney test for quantitative variables.
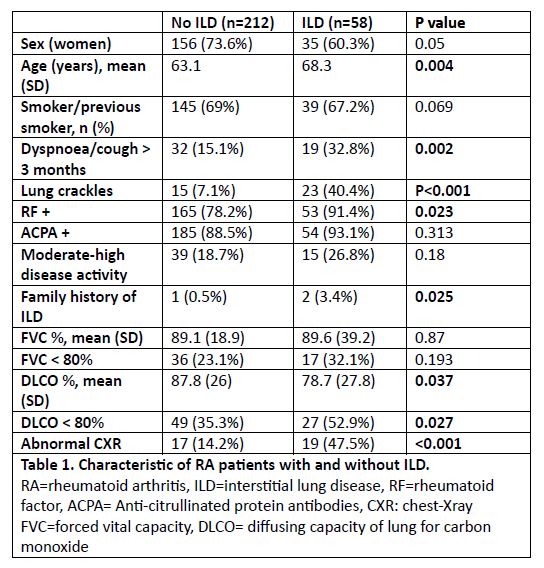
Results: A total of 270 patients with RA and a CT were included, and 58 patients (21.5%) had ILD. The patient’s characteristics are represented in table 1. A total of 204 (75.6%) patients had PFT and 160 (59.3%) had CXR performed. In the bivariate analysis, we observed a significant difference between patients without ILD and patients with ILD for abnormal CXR (14.2% vs 47.5%, p< 0.001) and DLCO< 80% (35.3% vs 52.9%, p=0.037). No significant differences were observed for FVC.The sensitivity and specificity for CXR, FVC< 80%, DLCO < 80% and the combined (abnormal CXR and/or abnormal PFT) results are represented in table 2. The best results were obtained for CXR due to high specificity, but sensitivity was low in all groups.
Conclusion: The diagnostic yield of CXR and PFT is low for ILD diagnosis, especially in patients without respiratory symptoms or lung crackles. Other strategies should be adopted for screening of ILD in patients with RA.
.jpg)
To cite this abstract in AMA style:
Loarce J, González Montes A, JIMENEZ BARRIOS S, Ferre-Sanfrancisco M, García García V, Bachiller J. Chest x-Ray and pulmonary function tests are not sensitive for screening intertitial lung disease in reumatoid arthritis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/chest-x-ray-and-pulmonary-function-tests-are-not-sensitive-for-screening-intertitial-lung-disease-in-reumatoid-arthritis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/chest-x-ray-and-pulmonary-function-tests-are-not-sensitive-for-screening-intertitial-lung-disease-in-reumatoid-arthritis/