Session Information
Date: Sunday, October 26, 2025
Title: (0731–0764) Vasculitis – Non-ANCA-Associated & Related Disorders Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Giant cell arteritis (GCA) is clinically heterogenous, and the presenting manifestations may influence diagnostic testing. The aim of this study was to evaluate the clinical manifestations of patients with GCA diagnosed by fluorodeoxyglucose (FDG) positron emission tomography (PET) / computed tomography (CT), and to compare PET-positive patients with those diagnosed with temporal artery biopsy (TAB).
Methods: A retrospective cohort of patients with GCA diagnosed by (FDG) PET/CT between 01/01/1990 and 12/30/2022 was assembled. The comparator cohort included patients with GCA diagnosed with temporal artery biopsy (TAB) at the same institution. The study was approved by the local Institutional Review Board (IRB). For statistical analysis, categorical variables were expressed as number (percentage) and continuous variables were expressed as mean (standard deviation) or median (interquartile range). Comparisons between cohorts were performed using chi-square and Kruskal-Wallis tests. A two tailed p value less than 0.05 was considered significant.
Results: The PET-positive cohort included 62 patients; demographics and baseline variables are presented in Table 1. Mean age was 70.1 years (SD 8.9), with 61% (38/62) female and 97% White (60/62). 71% (44/62) of patients met the 2022 ACR Classification Criteria for GCA. 65% (24/37) patients had a positive CT angiogram, and 67% (14/21) patients had a positive magnetic resonance angiogram (Table 2). A minority of patients underwent TAB, with 39 % (9/23) positive. Aortic ectasia and/or aneurysms were present in 24% (15/62) patients at diagnosis. 23% (14/62) patients had an abnormal FDG uptake consistent with polymyalgia rheumatica.The comparator cohort included 286 patients with TAB-positive GCA (Table 3). Compared to patients with TAB-positive GCA, the PET-positive patients were significantly younger (p< 0.001), more often males (p=0.036) and had longer time from symptom onset to GCA diagnosis (p< 0.001). PET positive patients had more frequent extremity claudication (p=0.026). Cranial manifestations were significantly less frequent among the PET-positive patients (p< 0.001), and none had permanent vision loss.
Conclusion: Patients with GCA diagnosed by PET scan were younger, more males and had less cranial manifestations compared to those diagnosed by TAB with a longer time to diagnosis. None of the patients diagnosed by PET had permanent vision loss. In clinical practice, distinct clinical GCA phenotypes tend to influence choice of diagnostic evaluation.
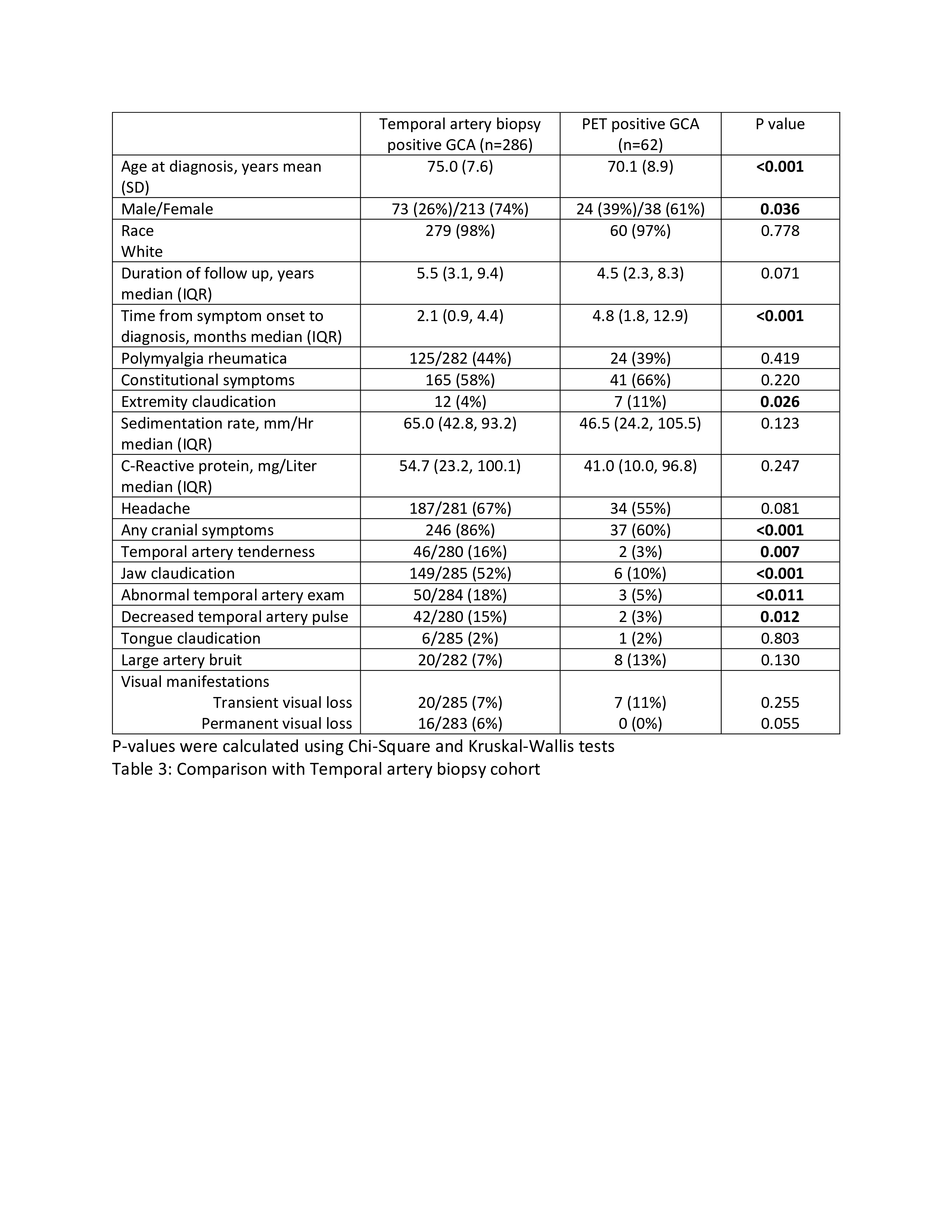 Table 1: Demographics and clinical characteristics
Table 1: Demographics and clinical characteristics
.jpg) Table 2: Imaging characteristics
Table 2: Imaging characteristics
.jpg) Table 3: Comparison with Temporal artery biopsy cohort
Table 3: Comparison with Temporal artery biopsy cohort
To cite this abstract in AMA style:
Mumtaz S, Clark L, Srivastava A, Langenfeld H, Hanson A, Crowson C, Abril A, Eshak N, Sullivan M, Koster M, Warrington K. Distinct differences between giant cell arteritis diagnosed by fluorodeoxyglucose (FDG) positron emission tomography (PET) versus temporal artery biopsy-a comparative cohort study [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/distinct-differences-between-giant-cell-arteritis-diagnosed-by-fluorodeoxyglucose-fdg-positron-emission-tomography-pet-versus-temporal-artery-biopsy-a-comparative-cohort-study/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/distinct-differences-between-giant-cell-arteritis-diagnosed-by-fluorodeoxyglucose-fdg-positron-emission-tomography-pet-versus-temporal-artery-biopsy-a-comparative-cohort-study/