Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Monitoring disease activity is a crucial aspect of the treat to target paradigm in the management of rheumatic diseases. There are no standardized protocols for monitoring disease activity levels in patients with Juvenile Idiopathic Arthritis (JIA) during the transition of care. The aim of this study is to compare different disease activity indices for all JIA category (excluding systemic JIA), to evaluate their discriminative validity in a real-life setting.
Methods: Young adult JIA patients eligible for transition of care underwent a prospective clinical evaluation by both paediatric and adult rheumatologists. Disease activity was assessed using validated clinical indices. The cJADAS, JADAS10, JADAS27, and JADAS71 were applied to all patients. SDAI, CDAI, and DAS28 were used for persistent oligoarticular (oJIA-p), extended oligoarticular (oJIA-e), and RF-positive and RF-negative polyarticular JIA (polyJIA RF-/RF+). The DAPSA was applied to patients with juvenile psoriatic arthritis (JPsA), while jSPADA, ASDAS-CRP, and BASDAI were used for patients with enthesitis-related arthritis (ERA). Ultrasound data were collected as an additional marker of articular inflammation in all cases of clinical suspicion of arthritis or for disease monitoring, to detect active synovitis according to OMERACT paediatric definitions. Spearman’s rank correlation was used to assess associations between the disease activity indices. ROC analyses were used to compare the ability of different clinical indices to reflect ultrasound-detected synovitis in selected JIA subgroups. Statistical analysis was performed using R software (version 4.5.0, released April 11, 2025; R Core Team).
Results: A total of 124 JIA patients were included (median age 19 years, IQR 17–23). Disease activity was highest in jPsA (Nf19; median JADAS10 3.8, DAPSA 5.0), compared to lower values in oJIA-e/polyJIA RF⁻ (JADAS10 2.5) and oJIA-p (JADAS10 3.0). In oJIA-p, oJIA-e, and polyJIA RF⁻, strong correlations were observed among JADAS scores, CDAI, and SDAI (ρ > 0.87; p < .001), with slightly lower values for DAS28. In the jPsA subgroup, a moderate-to-strong correlation was observed between JADAS scores and DAPSA (ρ ≈ 0.87, p < .001). In ERA, jSpADA correlated moderately with ASDAS-PCR (ρ = 0.51; p = 0.161), but not with BASDAI. Ultrasound was performed in 84.7% of patients, with a total of 1612 assessed joints. In oJIA-e and polyJIA RF⁻, JADAS71-PCR and SDAI yielded the highest AUCs (0.844–0.845) for ultrasound-detected synovitis. In oJIA-p, all indices performed well (AUCs ≥ 0.926). In jPsA, DAPSA showed the best discrimination (AUC 0.818).
Conclusion: In this real-life transition cohort, both paediatric (JADAS scores and jSPADA) and adult-derived indices (SDAI, CDAI, DAPSA, ASDAS-PCR, BASDAI) showed good correlation and comparable performance in assessing disease activity, in all JIA subtypes. These findings support the integration of selected adult indices into transitional care to ensure consistent and reliable disease monitoring.
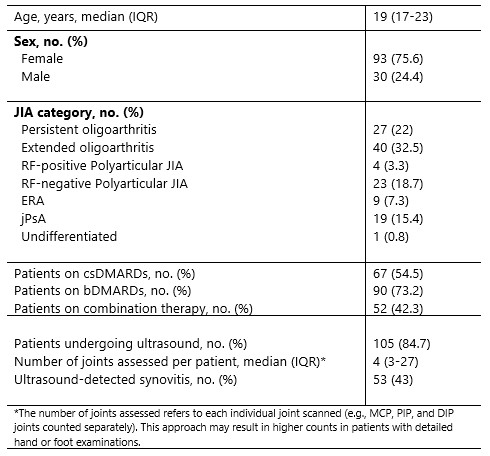 Table 1. Demographic and clinical characteristics of the study cohort (total N = 124)
Table 1. Demographic and clinical characteristics of the study cohort (total N = 124)
.jpg) Table 2. Summary of Disease Activity indices by JIA category. Values are expressed as median (IQR), except where indicated. RF: rheumatoid factor; PCR: C-reactive protein.
Table 2. Summary of Disease Activity indices by JIA category. Values are expressed as median (IQR), except where indicated. RF: rheumatoid factor; PCR: C-reactive protein.
.jpg) Table 3. Comparison of AUC values of the Disease Activity indices by JIA subgroups.
Table 3. Comparison of AUC values of the Disease Activity indices by JIA subgroups.
To cite this abstract in AMA style:
Pilato A, Tarantino G, Petrone M, Aquilani A, Marasco E, Nicolai R, De Benedetti F, Giacomelli R, Navarini L, Magni-Manzoni S. Which score fits best? Correlation of clinical indices of Disease Activity and Ultrasound findings in Juvenile Idiopathic Arthritis during Transitional Care [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/which-score-fits-best-correlation-of-clinical-indices-of-disease-activity-and-ultrasound-findings-in-juvenile-idiopathic-arthritis-during-transitional-care/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/which-score-fits-best-correlation-of-clinical-indices-of-disease-activity-and-ultrasound-findings-in-juvenile-idiopathic-arthritis-during-transitional-care/