Session Information
Date: Tuesday, November 19, 2024
Title: Abstracts: RA – Treatment II: Refining Use of Established Therapies
Session Type: Abstract Session
Session Time: 11:00AM-12:30PM
Background/Purpose: Glucocorticosteroid (GC) use is associated with increased mortality risk, especially from cardiovascular diseases (CVD) and infections, with dose and duration of use influencing risk. How long the impact lasts after stopping GC, and how this is influenced by duration of previous use, are not known. This study aims to estimate how the risk of mortality from CVD and infections is associated with i) cumulative duration of past GC use and ii) time since cessation of GC.
Methods: We conducted a longitudinal study of a population-based incident RA cohort, using administrative health data in a universal health care system. All incident RA cases in British Columbia, Canada, who met RA definition between 01/01/1996 and 12/31/2013, using a 5 yr look back period, were identified using physician billing data and followed until 12/31/2018. Oral GC exposure was measured as time-varying variables representing: current use, total cumulative duration of use, and time since discontinuation. Deaths with CVD or infections as the primary cause were identified from death certificates. Each incident user of GC was followed from time of starting GC (if started after RA index date) or of meeting RA criteria (if GC started before RA index date), using delayed entry to avoid immortal time bias, until death or censoring due to moving out of province or end of F/U. Multivariable conventional Cox PH model and its flexible extensions with non-linear effects were used to estimate the risk of death associated with cumulative duration of GC use, time since GC cessation and time varying interactions between the 2, adjusting for potential confounders (sociodemographic and comorbidities measured at index date and other RA meds as time-varying covariates).
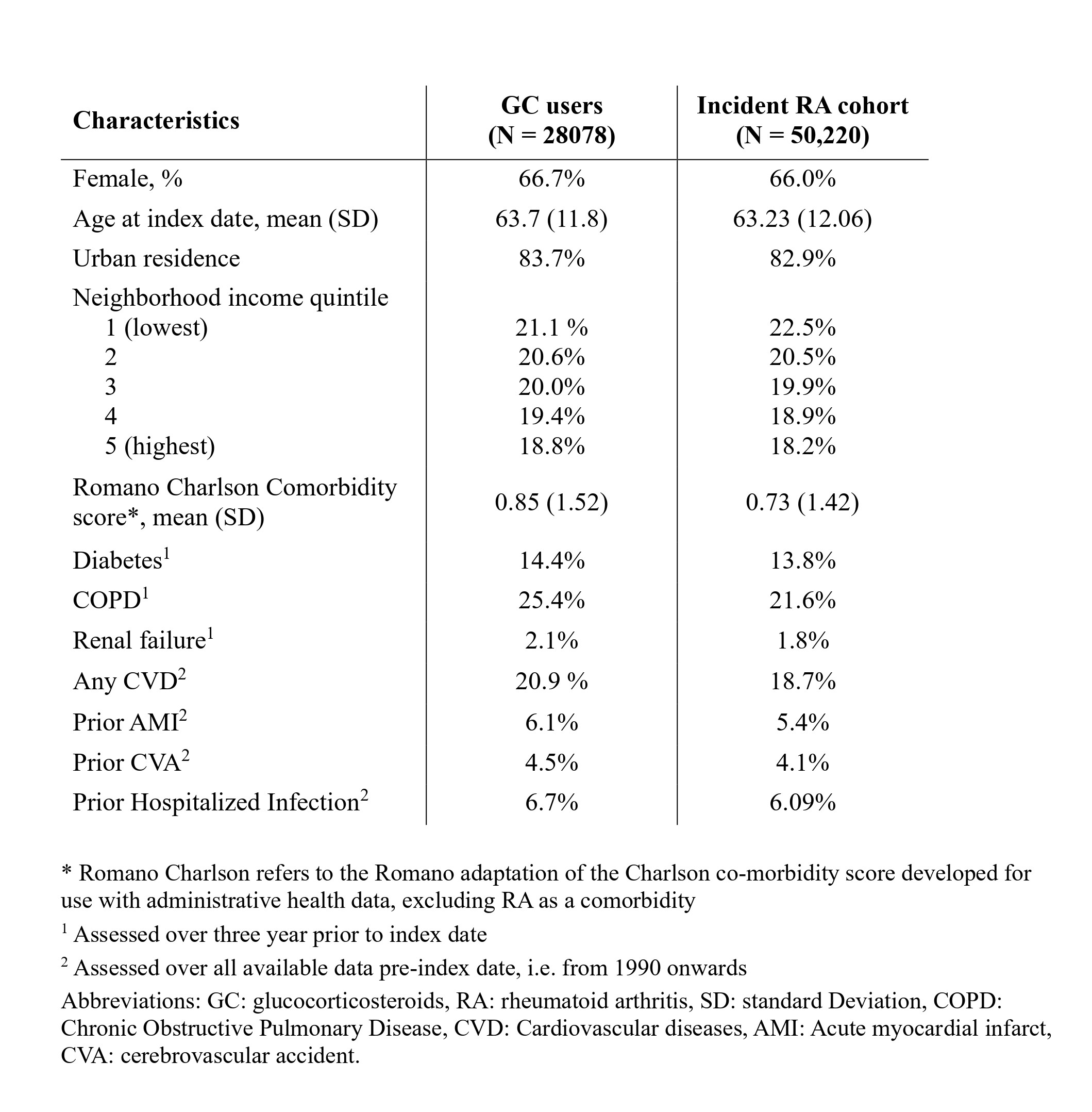
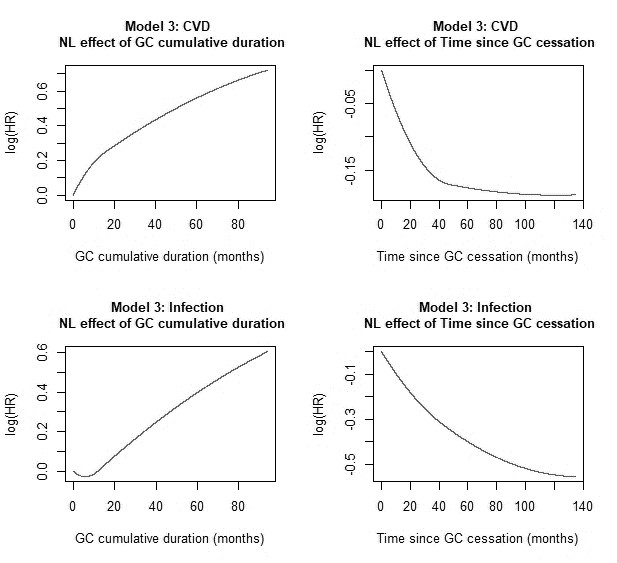
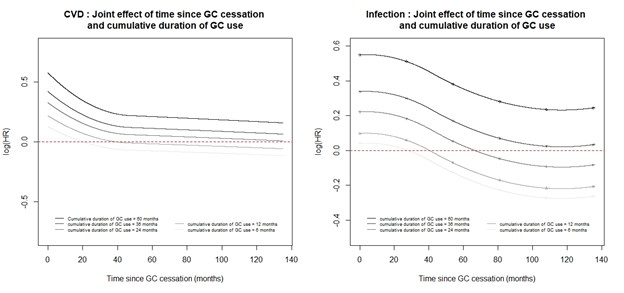
Results: We identified 28,078 incident GC users (55.9% of cohort), with mean (SD) and median (25;75Q) GC use duration of 603 (1116) and 131(18;598) days. See Table 1 for sample characteristics. We observed 2,489 CVD deaths and 387 from infections. In conventional Cox PHM risk of CVD / infection mortality increased by 7.5% / 6.8% for every year of GC use; and decreased by 1.3% / 4.9% for every year after stopping GC. Flexible extensions revealed non-linear relationships for both variables (Figure 1). Duration of previous use influenced risk after cessation (Figure 2). Risk decreased to that of someone prior to starting GC at 1.5, 3.5 and 10 years after cessation if GC had been used for 6,12, and 24 months for CVD deaths and at 2.5, 3.5, and 5.5 years, resp. for deaths from infections. Risk of death from CVD and infections never returned to pre-GC use risk in patients who used GC for > 2 years and > 3 years, respectively.
Conclusion: Despite advances in RA therapy GC are still commonly used and for long periods in some. The increased mortality risk from CVD and infections lasts for a substantial time after cessation, and never returns to that pre-GC with prolonged use. These findings are of high clinical relevance to people with rheumatoid arthritis and physicians, inform shared decision-making for starting and stopping GC, and provide evidence in support of RA guidelines recommending use of GC at lowest dose for shortest periods possible.
To cite this abstract in AMA style:
Lacaille D, Danieli C, Moolooghy K, Abrahamowicz M. Changes in Mortality Risk After Stopping Glucocorticosteroids – a Population-based Study in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/changes-in-mortality-risk-after-stopping-glucocorticosteroids-a-population-based-study-in-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/changes-in-mortality-risk-after-stopping-glucocorticosteroids-a-population-based-study-in-rheumatoid-arthritis/