Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Damage is irreversible and represents a permanent loss in organ function. Outcome measures are critical for minimizing and prevent damage acquisition. There are two damage scores for Sjogren syndrome (SS) – the Sjogren Syndrome Disease Damage Index (SSDDI), and the Sjogren Syndrome Damage Index (SSDI) with six and 10 domains respectively. Few studies have described damage accrual in primary SS (pSS) and none of them have compared these scores in the same population. The aim of this study was to characterize damage in a pSS cohort, comparing the SSDDI and SSDI indices in the same patients.
Methods: This was a single-center retrospective cohort study including patients with pSS followed-up in a tertiary hospital until February 2023. SSDDI and SSDI scores were assessed annually from the time of diagnosis. Events lasting ≥6 months or resulting in permanent loss of organ function/structure were considered to be damage. Categorical and continuous variables were compared using Chi-square and Student’s t test or Mann-Whitney U test when appropriate. SSDDI and SSDI scores were compared according to domains using two sample test of proportions. A p-value < 0.05 was considered significant.
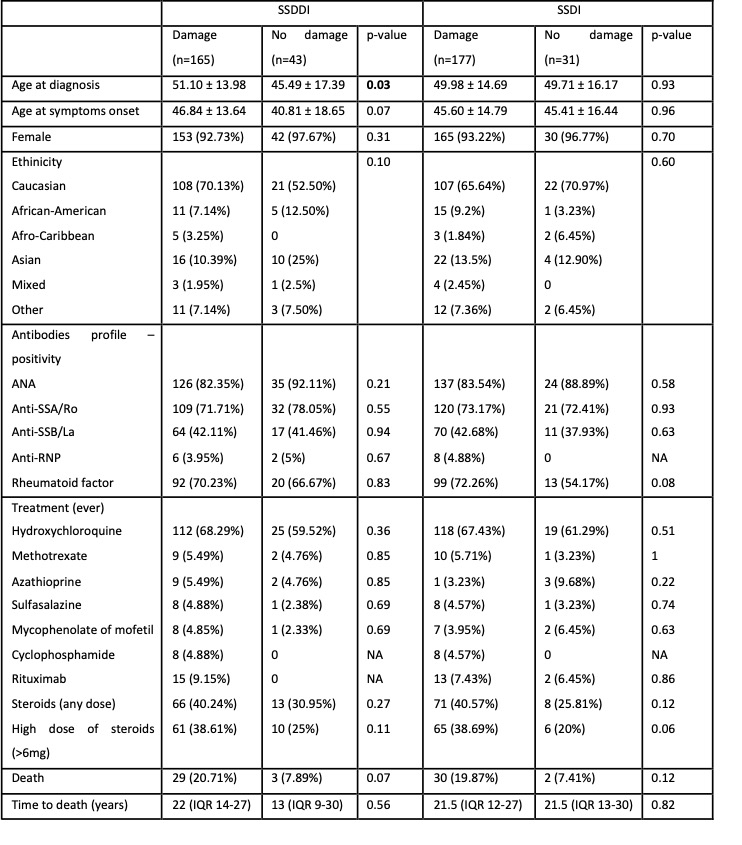
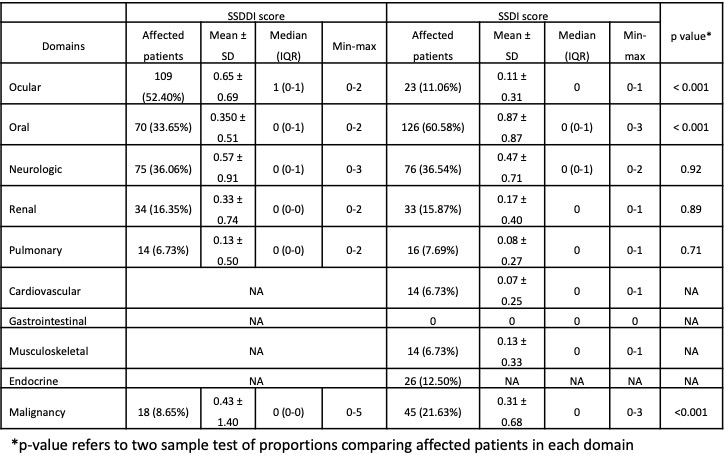
Results: We identified 208 patients with pSS followed for a mean of 14.1 ± 9.2 years. Most patients were female (93.8%) and Caucasian (66.49%). The median age at diagnosis was 49.9 ± 14.9 years, and 45.6 ± 15.0 years at symptom onset. Damage (at least one point) was observed in 165 (79.3%) and 177 (85.1%) patients, by the SSDDI and SSDI scores, respectively. Demographic and clinical features were similarly distributed between patients with and without damage (Table 1), the exception being the age at diagnosis, which was significantly higher in patients with damage according to the SSDDI (51.1 ± 14.0 vs. 45.5 ± 17.4 years; p=0.03) but not the SSDI. Ocular (52.4%), oral (33.7%) and neurologic (36.1%) were the most affected domains when using the SSDDI score, while oral (60.6%), neurologic (36.5%) and malignancy domains (21.6%) were more prevalent when using the SSDI score. Ocular domain impairment was more prevalent using the SSDDI than the SSDI (52.4% vs 11.1%). Compared to the SSDDI, the prevalence of impairment in the oral domain (33.7% vs 60.6%) and malignancy (8.7% vs 21.6%) were significantly higher when using the SSDI. Both scores identified similarly neurologic, renal, and pulmonary damage (Table 2).
Conclusion: SSDDI and SSDI scores are important tools when assessing damage in pSS patients. The distinct pattern of damage domain commitment is likely the result of different items included in each domain and differential weighing in the score.
To cite this abstract in AMA style:
Abrantes A, Gaspar P, Isenberg D. Characterization of Damage in a Primary Sjogren’s Syndrome Cohort [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/characterization-of-damage-in-a-primary-sjogrens-syndrome-cohort/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/characterization-of-damage-in-a-primary-sjogrens-syndrome-cohort/