Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: We aimed to assess whether sex, comorbidity and postoperative complications are associated with in-patient mortality after primary total knee arthroplasty (TKA) for osteoarthritis (OA).
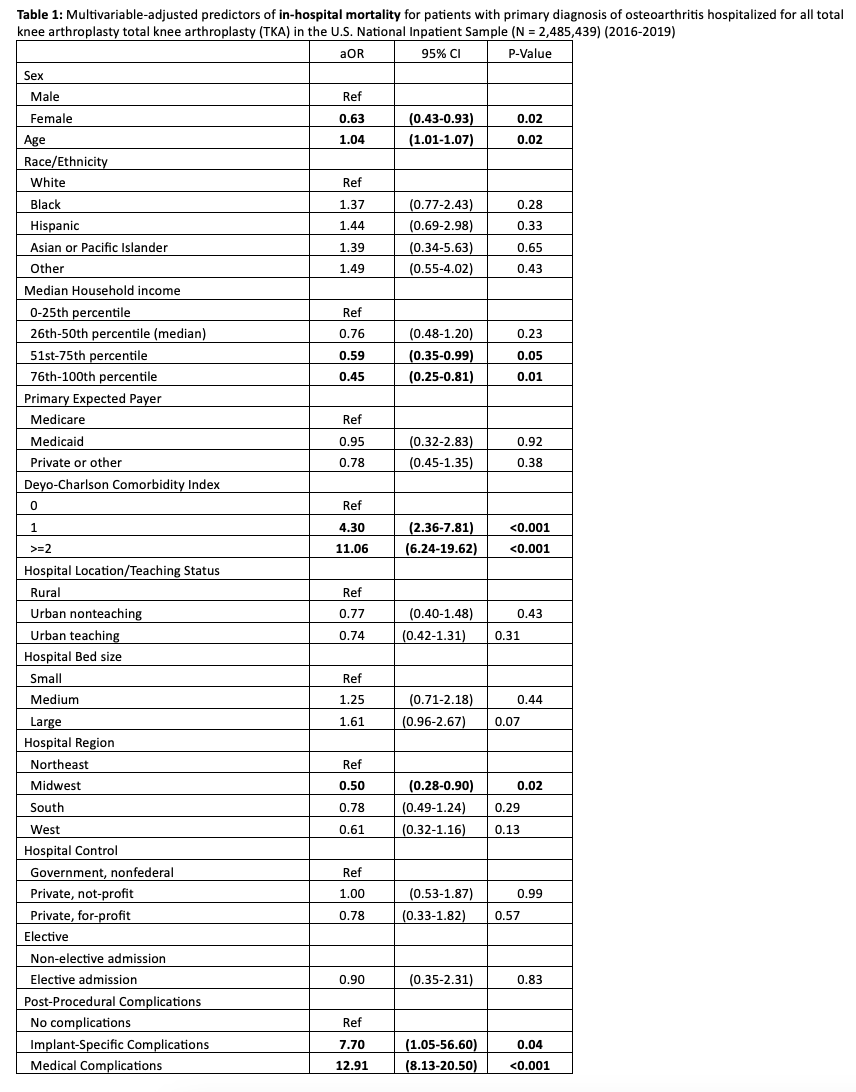
Methods: We used the 2016-2019 U.S. National Inpatient Sample (NIS), a nationally representative dataset. We calculated adjusted odds ratios (aOR) and 95% confidence intervals (CI) of the association of sex with in-hospital mortality after elective primary TKA for OA, adjusting for age, race/ethnicity, comorbidity, income, insurance payer, elective admission status, hospital characteristics (bed size, location/teaching status, region, control), and post-procedural complications (separated into implant-specific and medical complications).
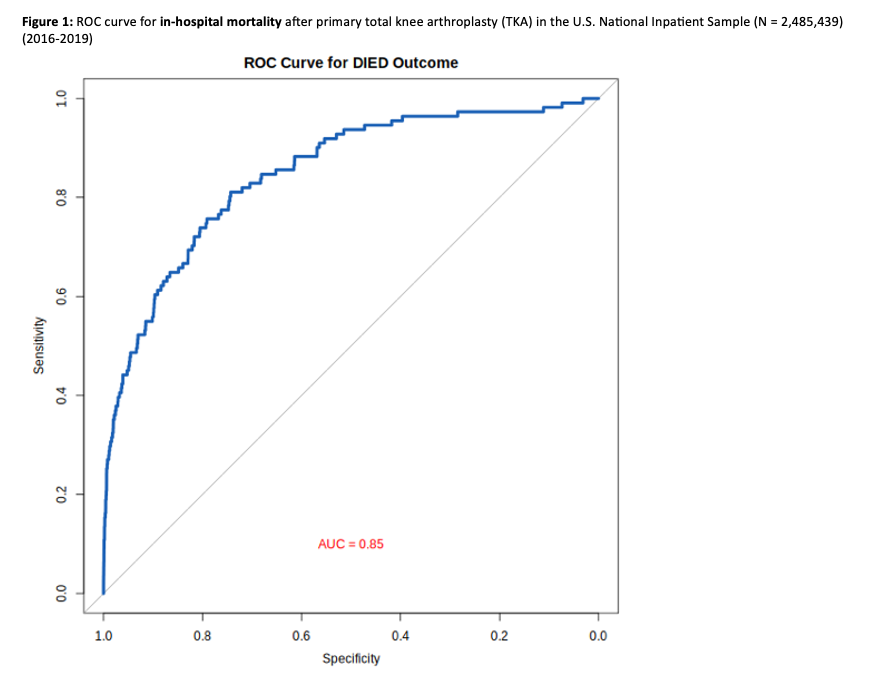
Results: We studied 2,627,960 primary TKA hospitalizations for OA from the 2016-2019 NIS. Females were more likely to be non-White, have lower Deyo-Charlson Comorbidity Index, more likely to have Medicare or Medicaid payer, and have post-procedure complications (p< 0.001 each). Other statistically significant differences in income and hospital characteristics (hospital bed size, location/teaching status, region, control) were small in magnitude (p< 0.001 each).In multivariable-adjusted analysis, we found that female sex was associated with a significantly lower in-hospital mortality, aOR was 0.63 (95% CI, 0.43 – 0.93; p=0.02) (Table 1). We also found that in-hospital mortality was significantly lower in subjects in the two highest quartiles of household income, and for hospitals located in the Midwest (p< 0.05 each). In-hospital mortality was significantly higher in people with Deyo-Charlson comorbidity index score of one or two or more, and both implant-specific and medical post-procedure complications, respective aORs were 4.30 (95% CI, 2.36-7.81; p< 0.001), 11.06 (95% CI, 6.24-19.62; p< 0.001), 7.70 (95% CI, 1.05-56.60; p=0.04), and 12.91 (95% CI, 8.13-20.50; p< 0.001). The final full multivariable-adjusted model that included post-procedural complications had a ROC curve area of 0.85 (95% CI, 0.81 to 0.89).
Conclusion: In a large in the U.S. national representative cohort of primary TKA for OA, male sex, medical comorbidity and post-procedure complications were associated with a significantly higher in-hospital mortality. Further studies into whether comorbidity-specific peri-operative management could be potential target to reduce mortality and complications are needed.
To cite this abstract in AMA style:
Chandrupatla S, Rumalla K, Singh J. Male Sex, Medical Comorbidity and Post-procedure Complications Are Associated with Higher In-hospital Mortality After Primary Total Knee Arthroplasty for Osteoarthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/male-sex-medical-comorbidity-and-post-procedure-complications-are-associated-with-higher-in-hospital-mortality-after-primary-total-knee-arthroplasty-for-osteoarthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/male-sex-medical-comorbidity-and-post-procedure-complications-are-associated-with-higher-in-hospital-mortality-after-primary-total-knee-arthroplasty-for-osteoarthritis/