Session Information
Date: Sunday, November 17, 2024
Title: Vasculitis – Non-ANCA-Associated & Related Disorders Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Current evidence shows that giant cell arteritis (GCA) is much more than a cranial disease, as it has a much broader and heterogeneous clinical spectrum than previously thought. Generally, it exhibits a typical clinical picture consisting of classic cranial ischemic manifestations but sometimes prevail non-specific clinical features related to the general inflammatory state or the extracranial large-vessel (LV) involvement.
Our study aims to investigate whether the distribution patterns of arterial involvement in 18F-FDG PET-CT differ between GCA with predominant cranial and extracranial phenotypes.
Methods: A retrospective review of 18F-FDG PET-CT findings in 140 GCA patients with vasculitis confirmed by temporal artery biopsy or imaging was conducted. Patients were divided into two groups: the predominant cranial group (with craniofacial ischemic manifestations during follow-up: headache, scalp tenderness, abnormal temporal artery examination, jaw claudication, visual symptoms) and the isolated extracranial GCA group (without evidence of craniofacial ischemic symptoms). The study was conducted under routine clinical practice conditions.
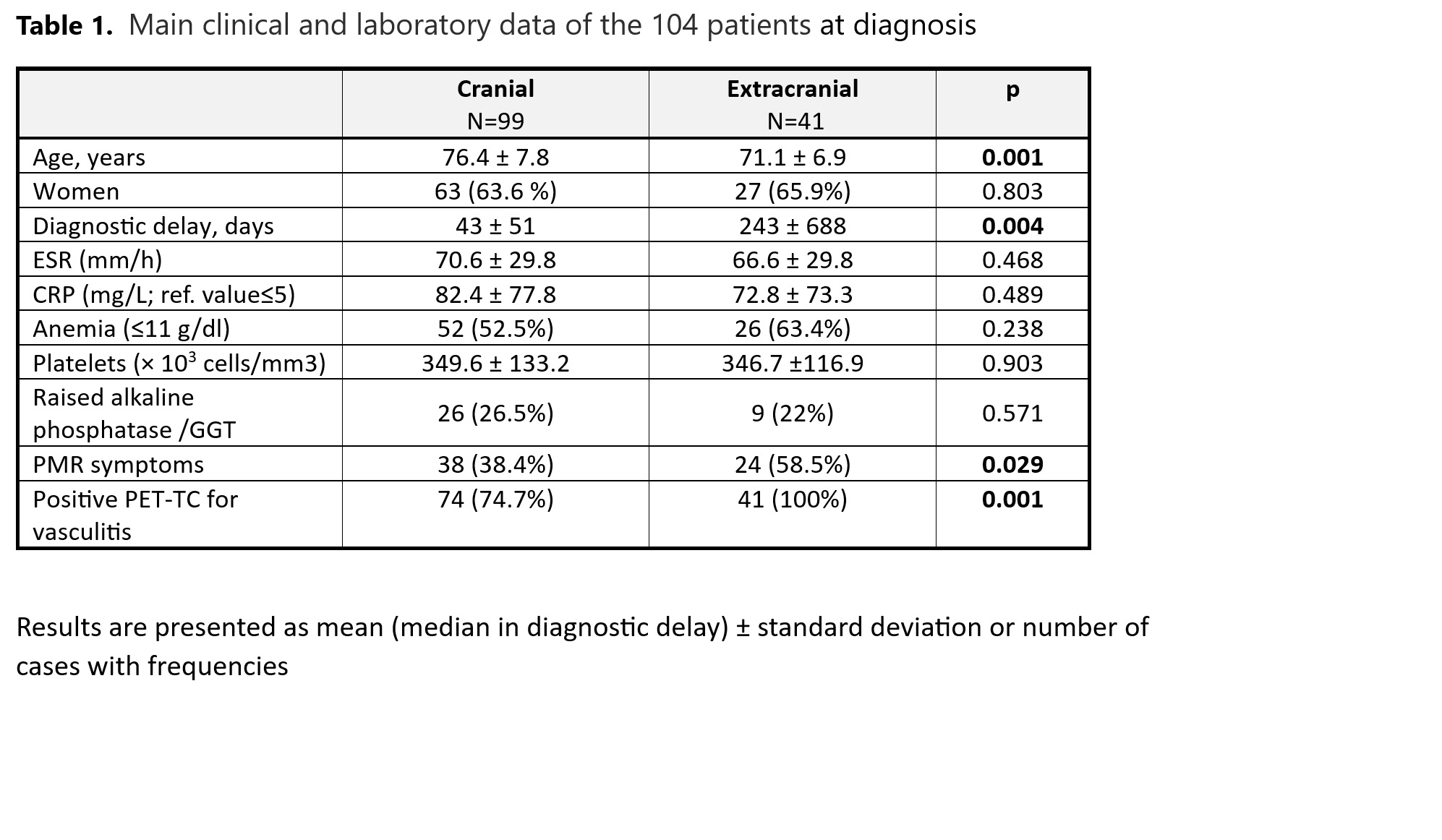
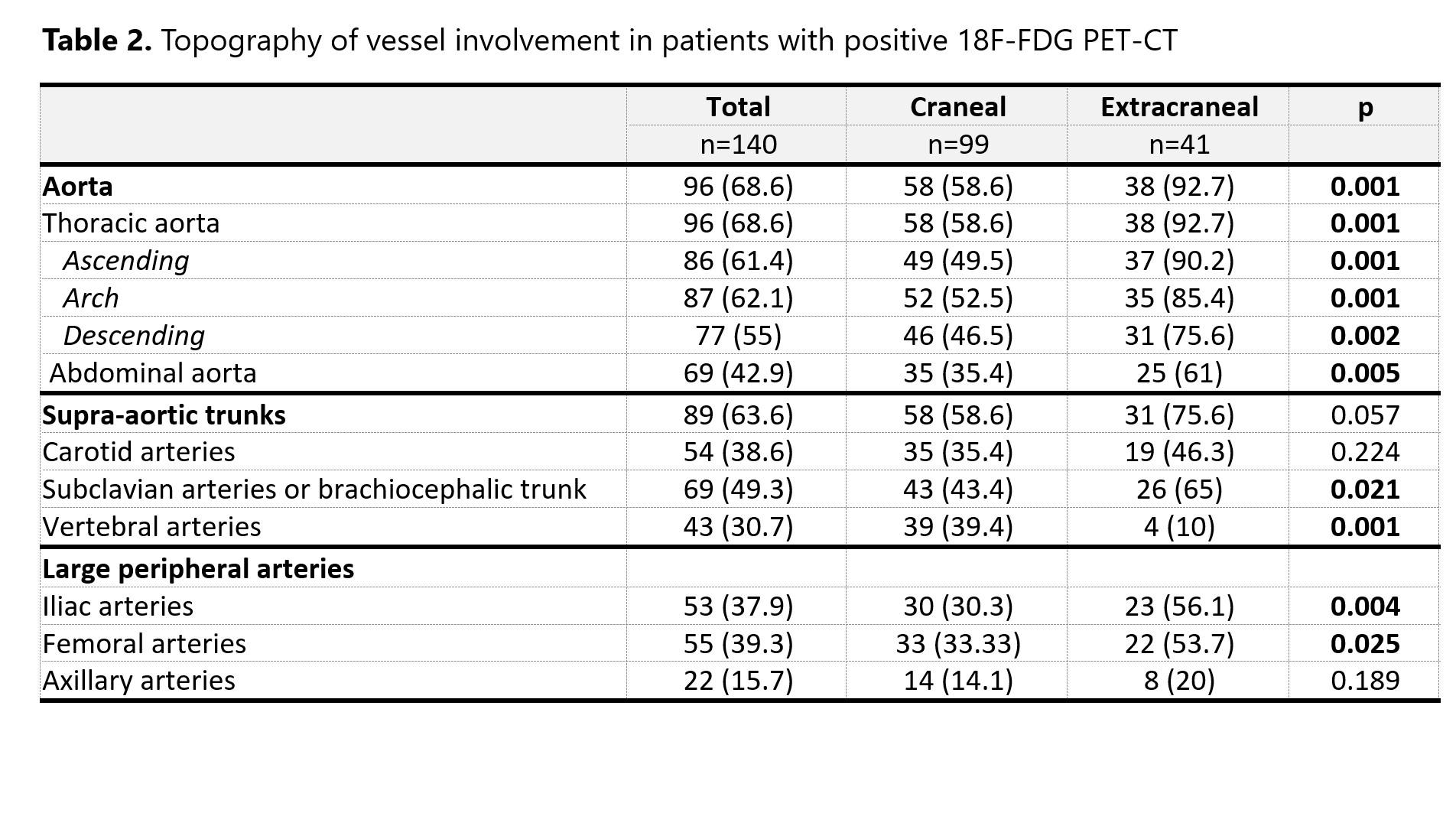
Results: Of the 140 patients (90 women), 99 (71%) had predominantly cranial GCA phenotype, while 41 (29%) had predominant extracranial GCA phenotype. The extracranial phenotype patients were notably younger (mean age ± SD: 71 ± 6.9 years vs. 76.5 ± 8 years; p = 0.001) and had a longer delay until diagnosis. In addition to disparities in craniofacial ischemic symptoms, they also presented polymyalgia rheumatica more frequently compared to those with a predominantly cranial GCA phenotype (58.5% vs. 38.4%, p = 0.029), and tended to exhibit less significant increases in acute phase reactant levels. When the arterial affection on 18F-FDG PET-CT was compared, we observed statistically significant differences (see table 2). A higher proportion of aortic involvement (in all segments of the thoracic aorta and the abdominal aorta) was observed in the extracranial phenotype, along with greater involvement of subclavian (65% vs 43.4%; p =0.021), iliac (56.1% vs 30.3%; p=0.004), and femoral arteries (53.7% vs 33.3%; p=0.025). In contrast, the cranial phenotype had a higher frequency of vertebral artery involvement (39.4% vs. 10%, p < 0.001).
Conclusion: Significant differences in the arterial involvement distribution patterns in 18F-FDG PET-CT were observed between GCA phenotypes. Patients with an extracranial phenotype exhibited a higher incidence of vasculitis in the aorta and extremity arteries. This accounts for atypical symptoms such as inflammatory lower back pain and limb claudication, and aligns with the increased risk of aortic aneurysm that has been reported.
To cite this abstract in AMA style:
Vidal p, Narvaez-García J, Sánchez-Rodríguez I, Sabaté-Llobera A, Cortés-Romera M, Palacios J, Maymó P, Roig Kim M, Aguilar Coll M, De Daniel L, Nolla J. Arterial Involvement Distribution on 18FFDG PET-CT in Giant Cell Arteritis: Variances Based on Clinical Phenotype [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/arterial-involvement-distribution-on-18ffdg-pet-ct-in-giant-cell-arteritis-variances-based-on-clinical-phenotype/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/arterial-involvement-distribution-on-18ffdg-pet-ct-in-giant-cell-arteritis-variances-based-on-clinical-phenotype/