Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Eosinophilic Granulomatosis with Polyangiitis (EGPA) is a rare autoimmune vasculitis of small to medium blood vessels, often causing multisystemic complications leading to increased morbidity and mortality. This study investigates various multisystemic complications among EGPA hospitalizations using the National Inpatient Sample (NIS) database.
Methods: Data from the NIS database 2016-2020 was utilized to identify all hospitalizations with a primary or secondary diagnosis of EGPA based on ICD-10 codes to include in the cohort. Demographic characteristics, length of hospital stay (LOS), and total hospital charges (THC) were analyzed. The prevalence of various complications was assessed and compared with non-EGPA hospitalizations. Chi-square and Wilcoxon rank sum tests were done using STATA 17.0 were used to determine significant differences, with a threshold set at p < 0.05. Odds ratios (OR) from logistic analyses were reported.
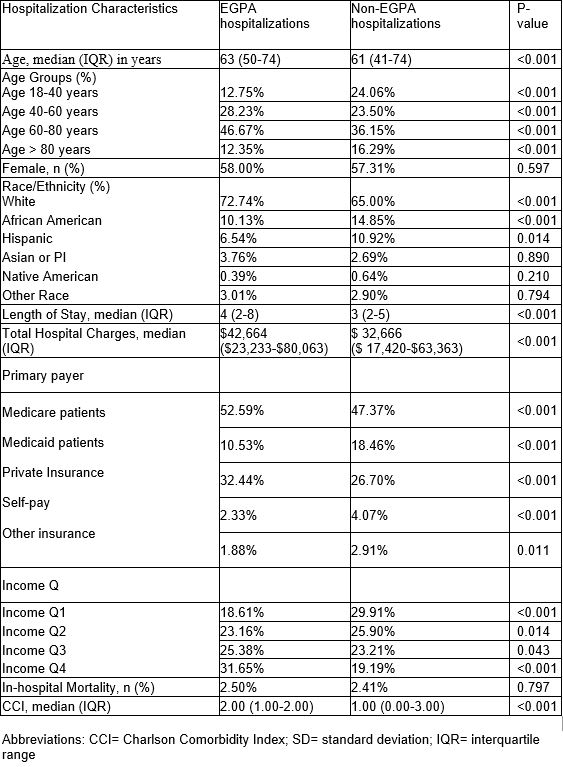
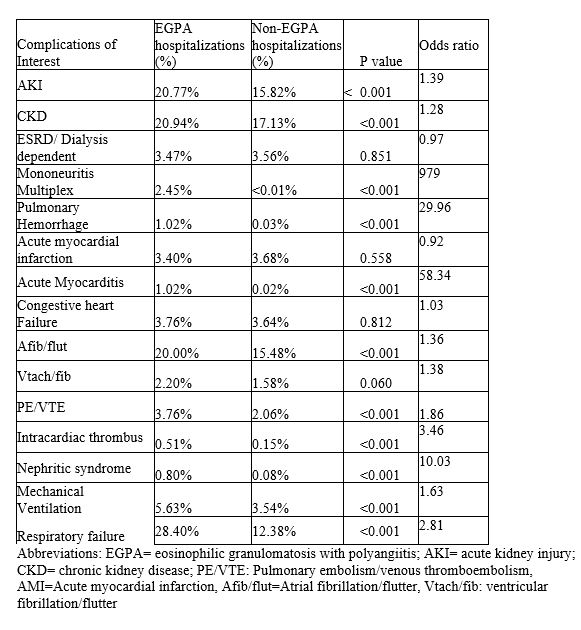
Results: A total of 8,785 EGPA hospitalizations were included. Patients had a median age of 63 years, with a majority aged 40-60 years (46.70%). Females accounted for 58.00% of the cohort, and 72.74% were White (p < 0.001; OR: 1.44), while African American and Hispanic patients were underrepresented compared to non-EGPA hospitalizations (Table 1). EGPA patients had a longer median LOS (4 days vs. 3 days; p < 0.001) and higher THC ($42,664 vs. $32,666; p < 0.001). Medicare was the primary payer for 52.6% (p < 0.001). They also exhibited a higher Charlson Comorbidity Index (2.00 vs. 1.00; p < 0.001). Complications that were more prevalent in EGPA included: Acute myocarditis (AM) (1.02% vs. 0.02%; p < 0.001; OR: 58.34), atrial fibrillation/flutter (Afib/flut) (20.00% vs. 15.48%; p < 0.001; OR: 1.36), intracardiac thrombus (IT) (0.51% vs. 0.15%; p < 0.001; OR: 3.46), acute kidney injury (AKI) (20.77% vs. 15.82%; p < 0.001; OR: 1.39), chronic kidney disease (CKD) (20.94% vs. 17.13%; p < 0.001, OR 1.28), mononeuritis multiplex (MM) (2.45% vs < 0.01%, p < 0.001, OR 979), pulmonary hemorrhage (1.02% vs. 0.03%; p < 0.001; OR: 29.96), pulmonary embolism/venous thromboembolism (PE/VTE) (3.76% vs. 2.06%; p < 0.001; OR: 1.86), nephritic syndrome (NS) (0.80% vs. 0.08%; p < 0.001; OR: 10.03), mechanical ventilation (5.63% vs. 3.54%; p < 0.01; OR: 1.63), and respiratory failure (28.40% vs. 12.38%; p < 0.001; OR: 2.81). No significant differences were found in ventricular tachycardia/ fibrillation (Vtach/fib), acute myocardial infarction (AMI), congestive heart failure (CHF), end-stage renal disease/dialysis-dependent (ESRD/DD), or inpatient mortality.
Conclusion: EGPA hospitalizations are characterized by longer stays, higher costs, and increased comorbidities compared to non-EGPA admits. They have significantly higher prevalence and odds of AM, Afib/flut, IT, AKI, CKD, MM, pulmonary hemorrhage, PE/VTE, NS, mechanical ventilation, and respiratory failure. These findings underscore the necessity of tailored care strategies for early complication detection and management in EGPA patients.
To cite this abstract in AMA style:
Sami F, Basharat A, Sami S, Tanveer S. Complications in Eosinophilic Granulomatosis with Polyangiitis (EGPA) Patients: A Nationwide Analysis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/complications-in-eosinophilic-granulomatosis-with-polyangiitis-egpa-patients-a-nationwide-analysis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/complications-in-eosinophilic-granulomatosis-with-polyangiitis-egpa-patients-a-nationwide-analysis/