Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: A 28 joint count of swelling (SJC), tenderness/pain on motion (TJC), and deformity/limited motion (DJC), is recommended to assess rheumatoid arthritis (RA) patient status. However, most visits of most RA patients do not include formal joint counts unless required for therapies. Furthermore, most current routine care and long-term databases omit DJC, which is unlikely to change with anti-inflammatory therapies, but which indicates progression and poorer patient status over 5 years, while SJC and TJC were unchanged (Arth Care Res. 1997;10:381). Another approach to assess RA patient status is for rheumatologists to estimate three 0–10 visual numeric scales (VNS) for inflammation (DOCINF), joint damage (DOCDAM), and patient distress (DOCDIS), in addition to physician global assessment (DOCGL), which requires 30 seconds compared to 90 seconds for formal joint counts. We compared SJC, TJC and DJC to DOCINF, DOCDAM, and DOCDIS in a cross -sectional study of RA patients with long disease duration.
Methods: A retrospective analysis was conducted of a cross-sectional study performed at a routine visit of RA patients which included 28 joint counts, (26 for SJC as shoulder swelling is not included), TJC and DJC, as well as a physician RheuMetric checklist to estimate DOCGL, DOCINF, DOCDAM, and DOCDIS. Cross-tabulations of SJC, TJC, and DJC as 0 or 1 vs ≥2, and DOCGL, DOCINF, DOCDAM, and DOCDIS as 0-2, 2.1-4, and >4 were analyzed using chi-square tests.
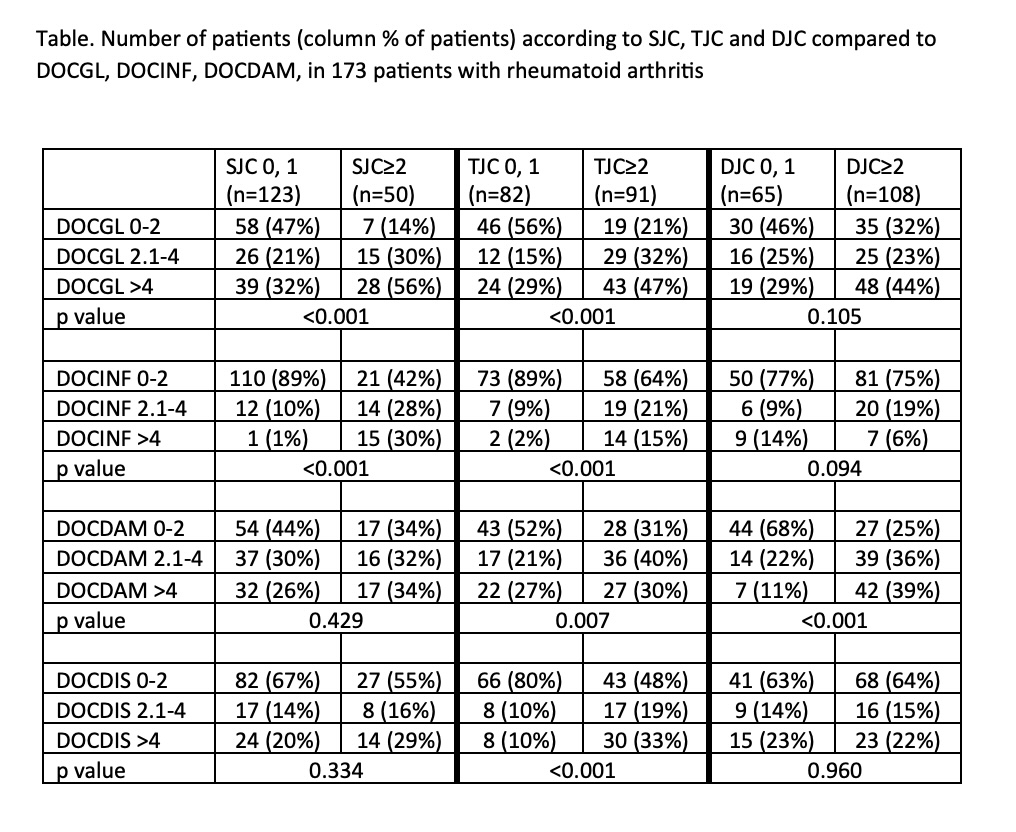
Results: The study included 173 patients with a median age of 61.3, and median disease duration of 10.0 years. Mean and median SJC were 1.7 and 0, TJC 3.8 and 2, DJC 5.4 and 4, DOCGL 3.7 and 3.5, DOCINF 1.5 and 1.0, DOCDAM 3.2 and 3.0 and DOCDIS 2.4 and 1.0, respectively. Two or more abnormal joints were seen in 29% of patients for SJC, 53% for TJC and 62% for DJC (Table). These findings indicate excellent control of inflammatory activity in current rheumatology care, as joint damage was more prominent than inflammation and patient distress in these RA patients managed over long periods. Overall, 47% of patients with 0 or 1 SJC had DOCGL 0–2 compared to 89% with DOCINF 0-2, 44% with DOCDAM 0-2 and 67% with DOCDIS 0-2 (Table). All comparisons of patients with TJC with DOCGL, DOCINF, DOCDAM, and DOCDIS were statistically significant, as TJC may indicate inflammatory activity, as well as joint damage and patient distress (Table). DJC was statistically significant only in comparisons with DOCDAM, Indicating specificity (Table). These data appear consistent with clinical observations and suggest face validity. Scoring of DOCGL, DOCINF, DOCDAM and DOCDIS required 25-30 seconds.
Conclusion: In RA patients with median disease duration of 10 years, TJC and DJC were higher than SJC, and DOCDAM and DOCDIS were higher than DOCINF, suggesting that joint damage and patient distress should be assessed in addition to inflammation in long-term clinical care of RA. DOCGL, DOCINF, DOCDAM and DOCDIS provide pragmatic quantitative assessment for routine care.
To cite this abstract in AMA style:
Pincus T, Li t, Schmukler J. Pragmatic Quantitative Rheumatologist 0–10 Visual Numeric Scale Estimates of Inflammation, Damage, and Patient Distress Have Face Validity and May Be as Informative as Formal 28 Joint Counts in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/pragmatic-quantitative-rheumatologist-0-10-visual-numeric-scale-estimates-of-inflammation-damage-and-patient-distress-have-face-validity-and-may-be-as-informative-as-formal-28-joint-counts-i/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/pragmatic-quantitative-rheumatologist-0-10-visual-numeric-scale-estimates-of-inflammation-damage-and-patient-distress-have-face-validity-and-may-be-as-informative-as-formal-28-joint-counts-i/