Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: CV disease is leading cause of morbidity and mortality in RA, largely due to endothelial dysfunction.1. Endothelial function is barometer of total cardiovascular risk while QRISK32 is a new risk assessment tool that is disease (includes RA) and ethnic specific to estimate 10-year risk of cardiovascular-disease. However, CV risk in RA is significantly related to the inflammatory disease activity but QRISK3 treats all RA patients similarly without taking into account the inflammatory disease burden. Endothelial function and related CV risk in RA is significantly related to inflammatory disease activity. However, the relationship between endothelial function and QRISK3 in RA remains unexplored.
Objectives:To elucidate the interplay between endothelial function and the 10-year risk of cardiovascular disease in RA.
Methods: 417 consecutive RA patients (371 females, 46 males; mean age: 53 ± 11 years; range: 25 to 82 years) meeting ACR/EULAR 2010 Rheumatoid Arthritis classification criteria on stable doses of cDMARDswere enrolled. Endothelial function was assessed using flow-mediated dilation (FMD) using AngioDefender. QRISK3 scores were calculated using demographic, clinical, and laboratory data, considering risk factors like age, ethnicity, deprivation, systolic BP, BMI, cholesterol, smoking, diabetes, hypertension, RA, atrial fibrillation, CKD, migraine, corticosteroids, and mental illness. QRISK3 classifies patients with score ˂10%as low risk, 10-20% as intermediate risk and >20% as high risk.Other disease specific variables: disease duration, ESR, CRP, DAS28& FMD%were also investigated for any possible correlation with QRISK3 score.Statistical analysis was performed using Graph Pad prism3 software. Correlation coefficients were calculated to assess the strength and direction of the correlation between FMD and QRISK3 scores.
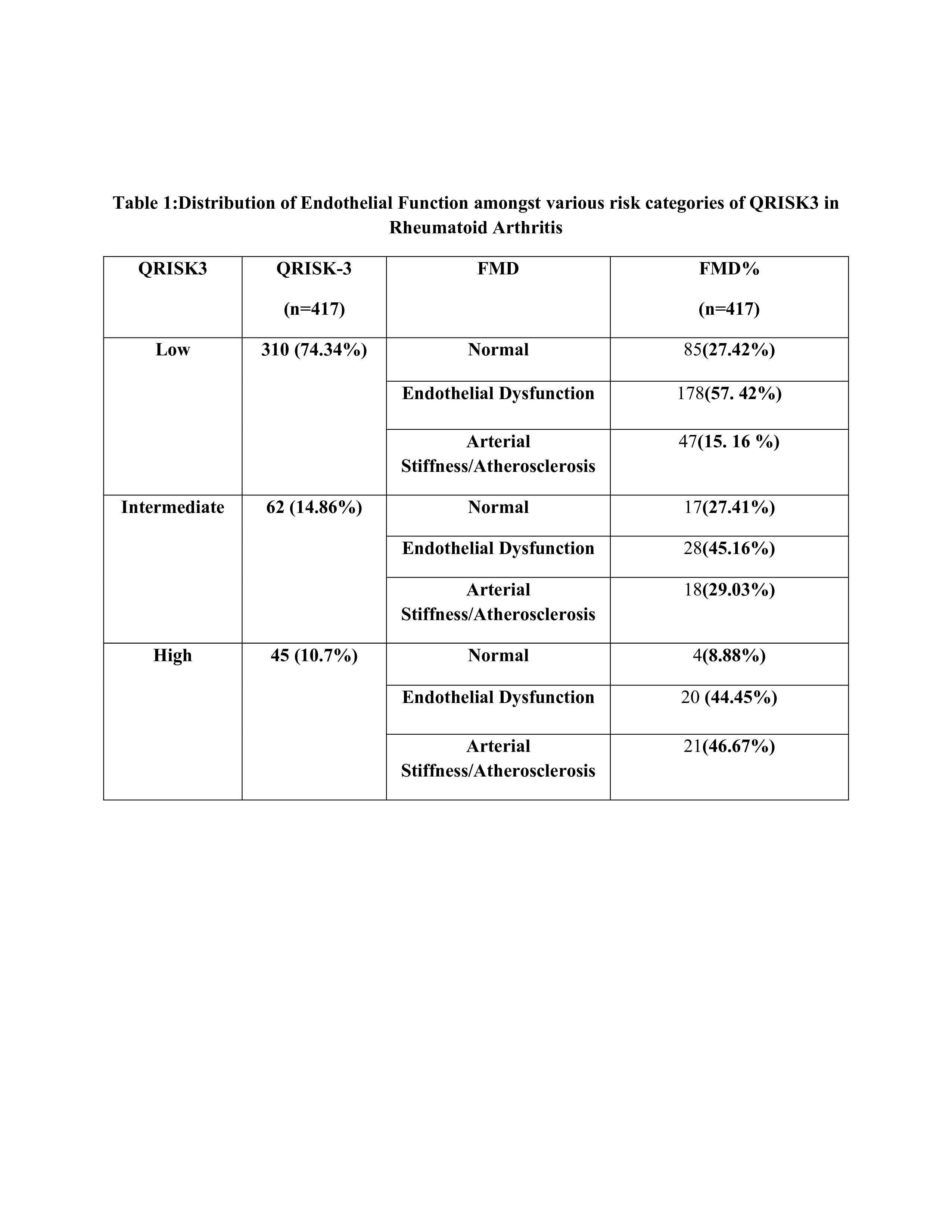
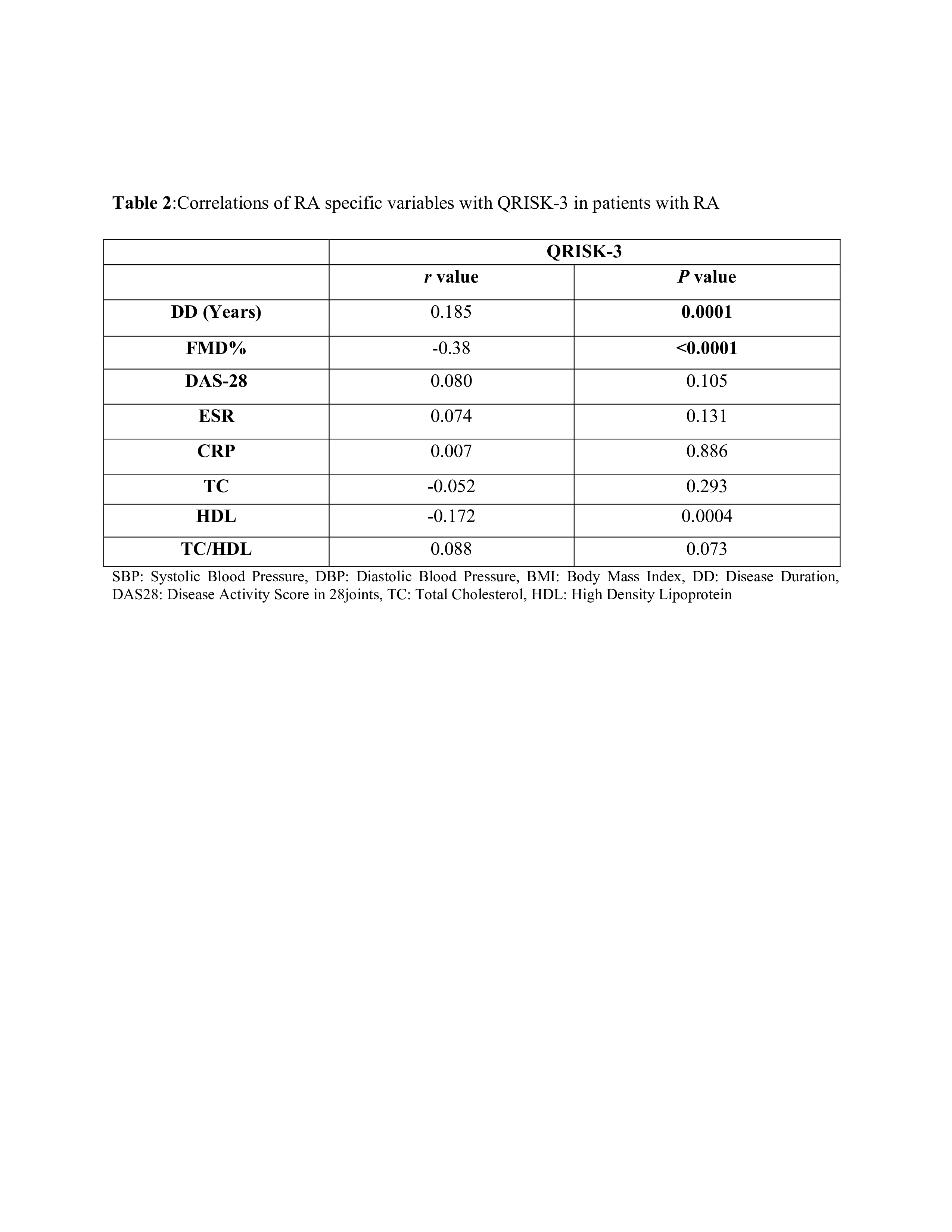
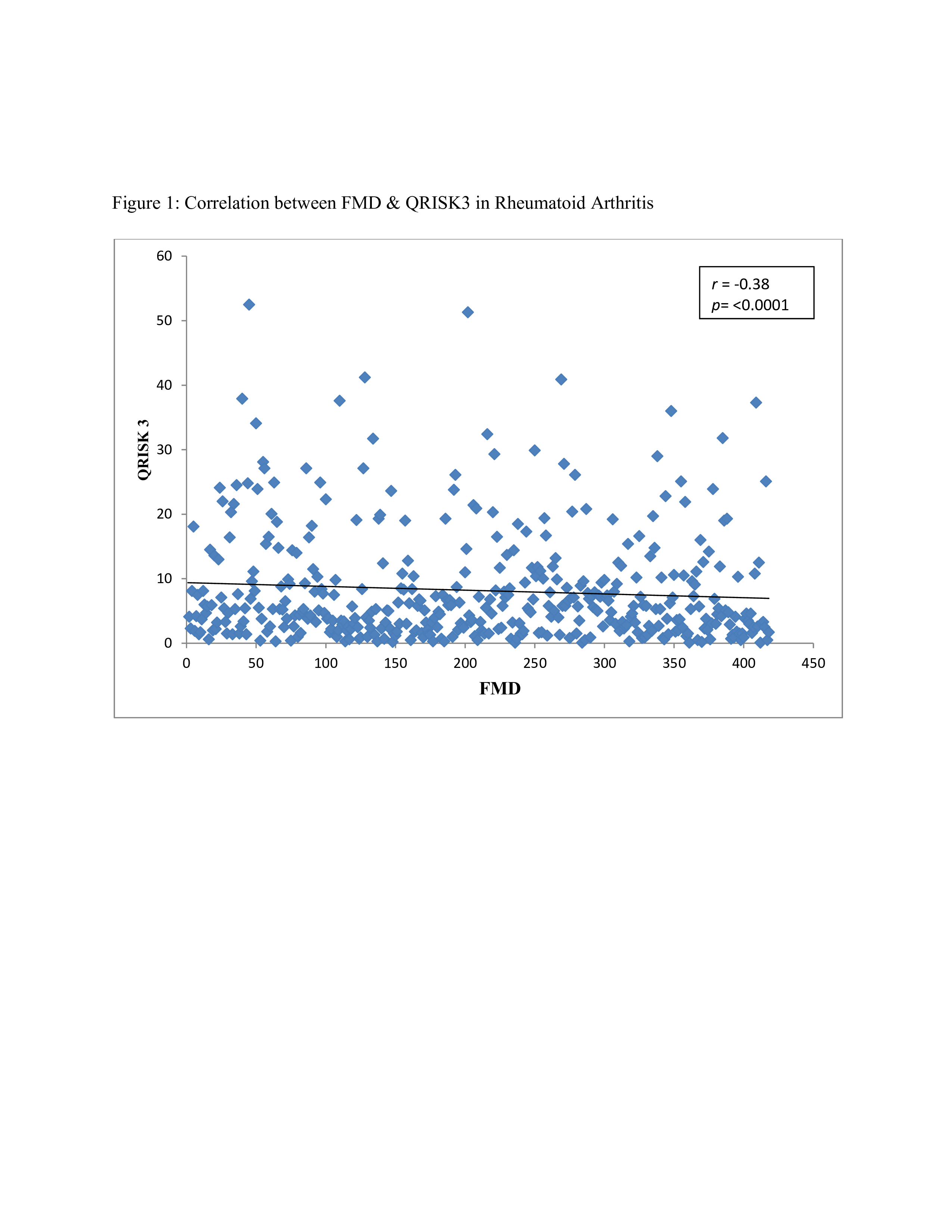
Results: Of the 417 recruited RA patients: 74.34% (n=310) had low, 14.86% (n=62) had intermediate and 10.7% (n=45) had high QRISK3 score. Of the patients with low (74.34%) QRISK3 score, 27.42% had normal FMD, 57.42% had endothelial dysfunction and 15.10% had arterial stiffness on FMD. Of the patients with intermediate (14.86%) QRISK3 score, 27.41% had normal FMD, 45.16% had endothelial dysfunction and 29.03% had arterial stiffness on FMD. Of the patients with high (10.7%) QRISK3 score, 8.88% had normal FMD, 44.45% had endothelial dysfunction and 46.67% had arterial stiffness on FMD (Table: 1). A significant inverse correlation was observed between FMD and QRISK3 scores (r = -0.38, p< 0.0001), indicating that impaired endothelial function was associated with higher 10-year cardiovascular risk (Fig: 1). Disease duration correlateddirectly while FMD% inversely correlated with QRISK3 estimated 10-year risk of cardiovascular disease. No other correlation was observed between disease specific variables and QRISK3 scores (table 2).
Conclusion: This the first study to ever demonstrate the inverse relationship between endothelial dysfunction and QRISK3 related to CV risk in RA. Further exploration of these correlations may refine risk stratification and guide targeted interventions for improved cardiovascular outcomes in RA.
To cite this abstract in AMA style:
Sabharwal V, Syngle A. Endothelial Dysfunction and QRISK3 in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/endothelial-dysfunction-and-qrisk3-in-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/endothelial-dysfunction-and-qrisk3-in-rheumatoid-arthritis/