Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: The 2021 American College of Rheumatology guidelines for treatment of rheumatoid arthritis (RA) conditionally recommend a gradual discontinuation of methotrexate (MTX) over biologic discontinuation. While MTX tapering may be a consideration for some patients, successful implementation will require understanding of patient and provider perspectives on methotrexate reduction. In this study, we aimed to evaluate the perspectives of patients and providers at different stages of practice on MTX tapering in stable RA at two tertiary care centers serving different patient populations.
Methods: After IRB approvals, Allegheny Health Network (AHN-urban) and Penn State Health (PSH-rural) rheumatology providers and RA patients at least 18 years old and on a stable dose of MTX for at least 6 months were surveyed on their perspectives about MTX use and taper. Patient surveys included questions about demographics, health history related to RA and MTX use, and views on tapering and discontinuation of MTX. Provider surveys included questions about years of experience, timing of tapering, and preferred strategies for tapering. All surveys were anonymous. Data were collected in REDCap. Chi square analysis and Wilcoxon rank sum tests were used to analyze stratified data.
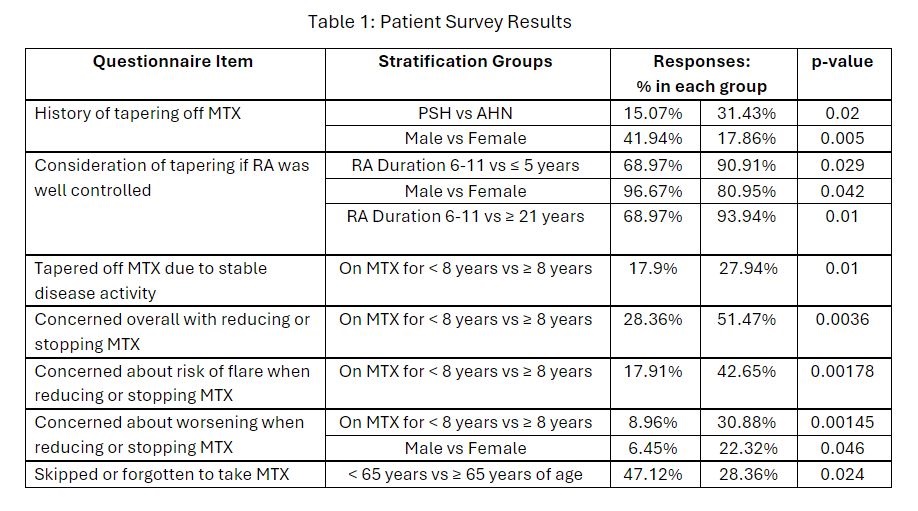
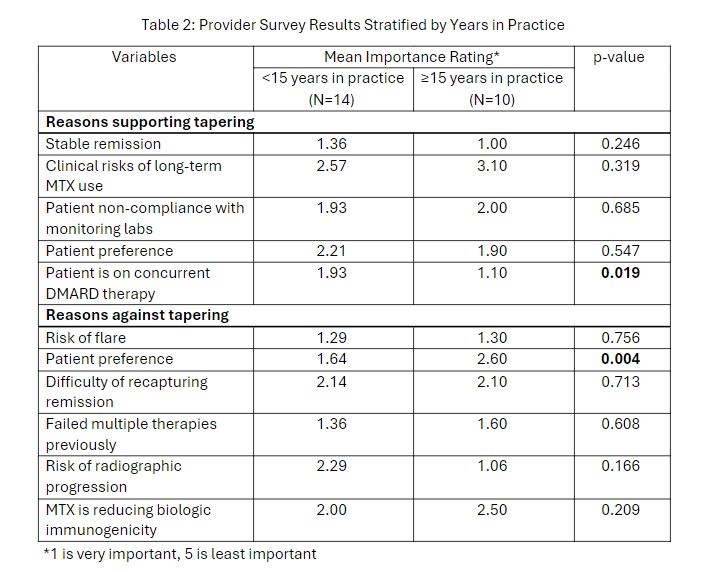
Results: Surveys were collected from patients: 73 at AHN and 70 at PSH. They included 112 females (78%) ; 86% were White. Duration of RA was >11 years in 52% and duration of MTX use was >7 years in 50%. Self-assessed RA status ( 0=very well and 10 = poor) was significantly better in White patients (mean score 3.41) than in non-White patients (mean score 5.06; p=0.007). In response to questions about MTX tapering, significant differences were noted in defined subgroups (Table 1). Tapering trials of MTX were more frequent at AHN than PSH (P=0.02) maybe related to medical co-morbidities, were more frequently attempted or considered in males than females (P=0.005, P=0.042, respectively) and in those with > 21 years of disease (P=0.01). Tapering off MTX was more frequent in patients on the drug for at least 8 years than those with < 8 years (P=0.01). However, concerns about risks of reducing or stopping MTX, including flares or worsening, were greater in patients on MTX for at least 8 years (P values 0.0036, 0.00178, 0.00145) and were also greater in females than males (P=0.046). The frequency of skipping MTX was greater in patients < 65 years of age than those older (P=0.024). Surveys were completed for 16 providers at AHN and 8 at PSH; 42% had been in rheumatology practice for ≥15 years (Table 2). Providers with < 15 years of experience were more likely to consider concurrent DMARD as favorable for tapering MTX (P=0.019) and were also more likely to consider patient preferences against tapering (P=0.004). No significant differences were found between the two provider networks (not shown).
Conclusion: In our multi-center study, we uncovered patient and provider factors that could influence tapering decisions, including age, race, sex, duration of RA, duration of MTX use, provider’s years of experience, and population-level differences between two different tertiary care centers. Consideration of these factors will facilitate decisions regarding MTX tapering in stable RA.
To cite this abstract in AMA style:
Newman P, Banks S, June R, Lehman E, Smith G, Rai V, Wilson N, Olsen N, Sharma T. Opinions from Rheumatoid Arthritis Patients and Providers on Discontinuing Methotrexate in Stable Disease [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/opinions-from-rheumatoid-arthritis-patients-and-providers-on-discontinuing-methotrexate-in-stable-disease/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/opinions-from-rheumatoid-arthritis-patients-and-providers-on-discontinuing-methotrexate-in-stable-disease/