Session Information
Date: Monday, November 13, 2023
Title: (1124–1154) Miscellaneous Rheumatic & Inflammatory Diseases Poster II
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Adult-Onset Still’s Disease (AOSD) commonly manifests with fever, arthritis, rash, liver dysfunction, lymphadenopathy, and hematologic abnormalities. AOSD is also associated with Hemophagocytic Lymphohistiocytosis (HLH). We aimed to study the characteristics and outcomes of adult AOSD hospitalizations with HLH, as well as independent predictors of inpatient mortality.
Methods: We utilized the 2016 to 2019 National Inpatient Sample (NIS) database to obtain hospitalizations with a principal or secondary diagnosis of AOSD. We subdivided AOSD hospitalizations into those with and without HLH. ICD-10 codes were used to identify diagnoses. Demographics, complications of interest, total hospital charges (THC) and length of stay (LOS) were collected and compared. Variables with a p value ≤ 0.2 in the univariable screen were included in a multivariable logistic regression model for in-hospital death. Results were reported as odds ratios (OR).
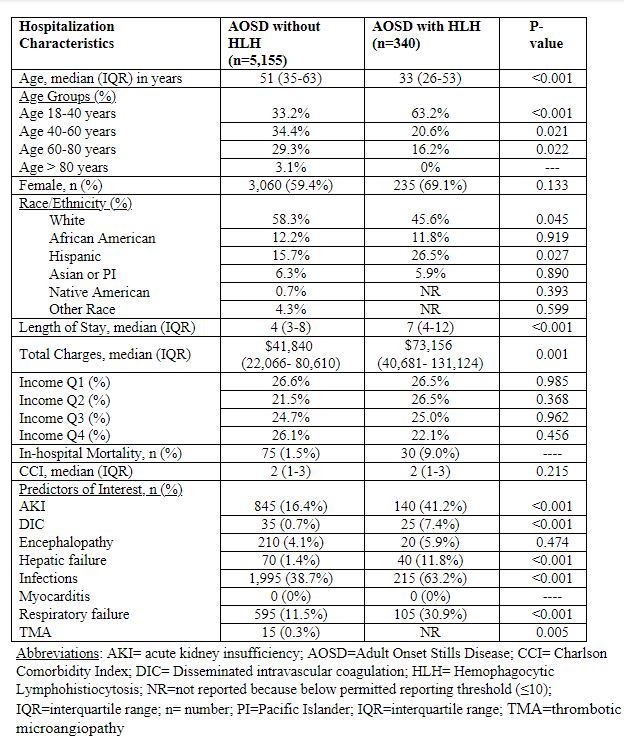
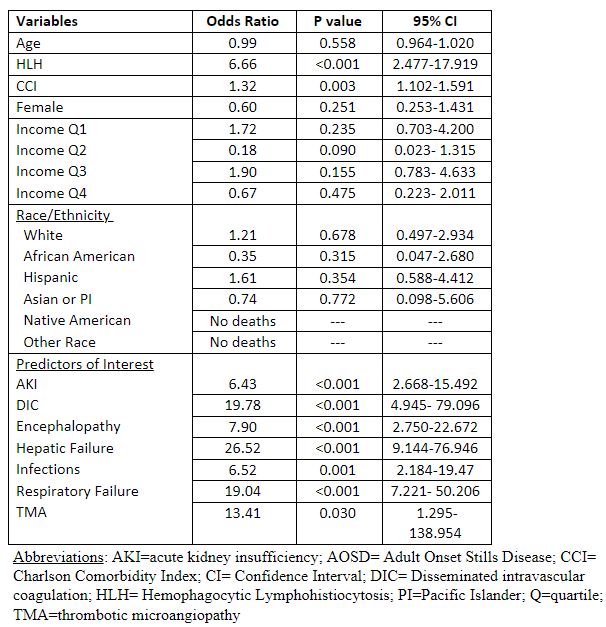
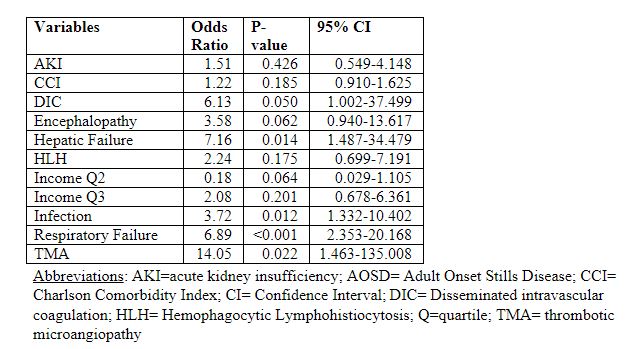
Results: We identified 5,495 adult AOSD hospitalizations, of which 340 (6.2%) had HLH, and 5,155 (93.8%) did not have HLH (table 1). Relative to the non-HLH group, HLH group was younger (median age 33 vs 51 years; p< 0.001), had similar percentage of females (69.1% vs 59.4%; p=0.133), had less whites (45.6% vs 58.3%; p=0.045), similar percentage of African Americans (11.8% vs 12.2%; p=0.919), but had more Hispanics (26.5% vs 15.7%; p=0.027), had longer median LOS in days (7 vs 4; p< 0.001) and a higher median THC ($73,156 vs $41,840; p=0.001). The HLH group had higher prevalence of acute kidney insufficiency (AKI) (41.2% vs 16.4%; p< 0.001), disseminated intravascular coagulation (DIC) (7.4% vs 0.7%; p< 0.001), hepatic failure (11.8% vs 1.4%; p< 0.001), infections/pneumonia/sepsis (63.2% vs 38.7%; p< 0.001), respiratory failure (30.9% vs 11.5%; p< 0.001), and thrombotic microangiopathy (TMA) (2.9% vs 0.3%; p=0.005). Univariable analyses for predictors of in-hospital mortality in AOSD hospitalizations are shown in table 2. Multivariable analysis showed that DIC (OR 6.13; 95% C.I. 1.002-37.499), hepatic failure (OR 7.16; 95% C.I. 1.487-34.479), infection/pneumonia/sepsis (OR 3.72; 95% CI 1.332-10.402), respiratory failure (OR 6.89; 95% C.I. 2.353-20.168) and TMA (OR 14.05; 95% CI 1.463-135.008) were associated with higher odds of in-hospital death among AOSD hospitalization (table 3).
Conclusion: We found that HLH only occurred in 6.2% of AOSD inpatients. Inpatients with both AOSD and HLH had a higher rate of concurrent AKI, DIC, hepatic failure, infections, respiratory failure, and TMA. They were also younger, had a higher proportion of Hispanics, longer LOS, greater total hospital charges, and a 9% in-hospital mortality in contrast to 1.5% in those without HLH. Despite a large difference in mortality between the groups, HLH itself was not found to be an independent risk factor for in-hospital death. Multivariable analysis in AOSD inpatients showed DIC, hepatic failure, infection/pneumonia/sepsis, respiratory failure, and TMA to be associated with higher odds of death. This information can help clinicians by improving awareness of these life-threatening complications since early recognition and prompt management may improve outcomes.
To cite this abstract in AMA style:
Sami F, Manansala M, Arora S, Manadan A. Nationwide Analysis of Adult-Onset Still’s Disease with and Without Hemophagocytic Lymphohistiocytosis [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/nationwide-analysis-of-adult-onset-stills-disease-with-and-without-hemophagocytic-lymphohistiocytosis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/nationwide-analysis-of-adult-onset-stills-disease-with-and-without-hemophagocytic-lymphohistiocytosis/