Session Information
Date: Sunday, November 12, 2023
Title: Abstracts: RA – Diagnosis, Manifestations, & Outcomes I: RA-ILD
Session Type: Abstract Session
Session Time: 2:00PM-3:30PM
Background/Purpose: RA-associated interstitial lung disease (ILD) is not a single entity as illustrated by different HRCT patterns, different risk factors and prognoses suggesting heterogenous phenotypes. Our objective was to identify definite sub-phenotypes among a large RA-ILD dataset performing unsupervised clustering analysis.
Methods: In this international collaborative study (22 centers from 13 countries), we included patients with RA (ACR/EULAR 2010 classification criteria) having ILD defined by high-resolution computed tomography (HRCT) chest scan. Clinical, biological, imaging, and functional data were retrospectively collected from extensive chart review. Missing data were handled using multiple imputation with chained equations. A multiple correspondence analysis was performed on each sample to reduce dimensions and a non-parametric Bayesian algorithm was used to attribute a cluster to each patient. The clusters were aggregated over the multiple imputations using weighted Non-negative Matrix Factorization.MUC5B rs35705950 T risk allele distribution in the identified clusters was investigate for patients with available genotype. A surrogate decision tree was conducted using the non-imputed dataset to predict a cluster for each patient. The prediction error rate of the tree was estimated using cross-validation.
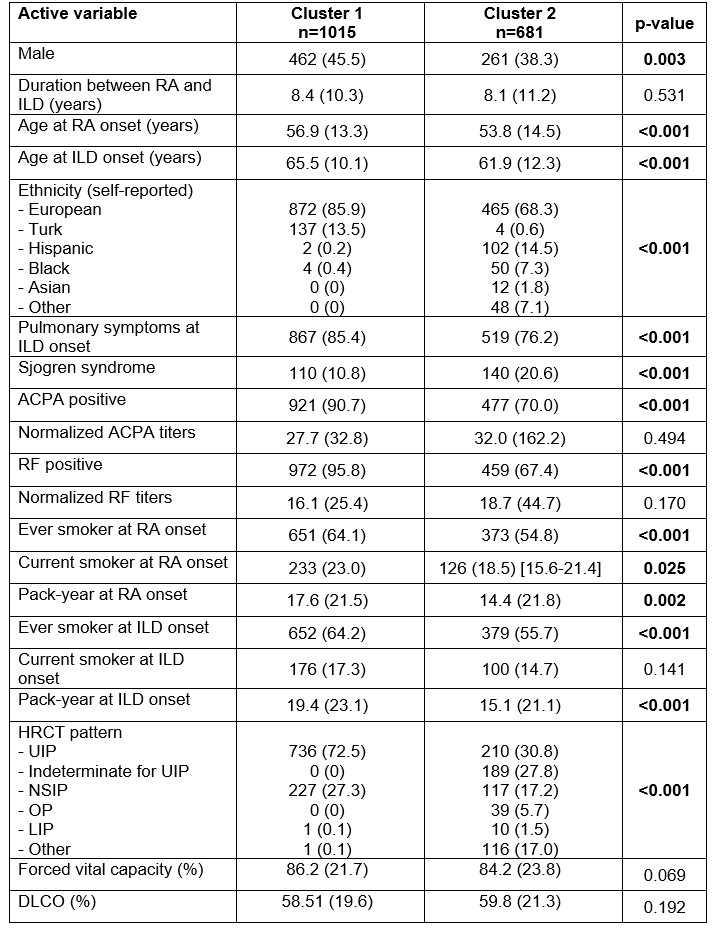
Results: A total of 1696 patients with RA-ILD were included in the cluster analysis; Table 1. Among the 37 collected variables, 20 active variables were used to construct clusters. The non-parametric Bayesian clustering algorithm detected 2 definite clusters: cluster 1 (n=1015) and cluster 2 (n=681); Table1, Figure 1. Compared to cluster 2, patients from cluster 1 were more frequently male (45.5% vs 38.3%, p=0.003), older at RA onset (56.9 ± 13.3 vs 53.8 ± 14.5, p< 0.001) and at ILD onset (65.5 ± 10.1 vs 61.9 ± 12.3, p< 0.001), more frequently with European ethnicity (85.9% vs 68.3%, p< 0.001), more frequently ever smokers at ILD onset (64.2% vs 55.7%, p< 0.001) and had less Sjogren syndrome (10.8% vs 20.6%, p< 0.001). They were more frequently positive for anti-citrullinated peptides antibodies (90.7% vs 70.0%, p< 0.001) and for rheumatoid factor (95.8% vs 67.4%, p< 0.001). UIP HRCT pattern was predominant in cluster 1 (72.5%) whereas various patterns were observed in cluster 2 (UIP = 30.8%, NSIP = 17.2%), p< 0.001. There was no difference in lung function at ILD onset between the 2 clusters. MUC5B rs35705950 genotype was available for 444 patient (26.2%) with a higher minor allele frequency (MAF) in cluster 1 (33% compared to 18%, p< 0.001). Figure 2 shows the decision tree that can be used to predict the cluster for a new patient with a prediction error rate of 9.8%.
Conclusion: Our results provide evidence that RA-ILD is a heterogeneous disease and allow the identification of at least two distinct subsets. This heterogeneity is illustrated by a contribution of the MUC5B promoter variant restricted to cluster 1, promoting the identification of specific risk scores for each RA-ILD subset. This heterogeneity underlies distinct physio pathological mechanisms which could influence not only the prognosis of patients with RA-ILD but also their therapeutic management.
ACPA: anti-citrullinated peptides antibodies; DLCO: diffusion capacity of the lung for carbon monoxide; HRCT: high-resolution computed tomography; ILD: interstitial lung disease; LIP: lymphocytic interstitial pneumonia; NSIP: non-specific interstitial pneumonia; OP: organizing pneumonia; RF: rheumatoid factor; UIP: usual interstitial pneumonia
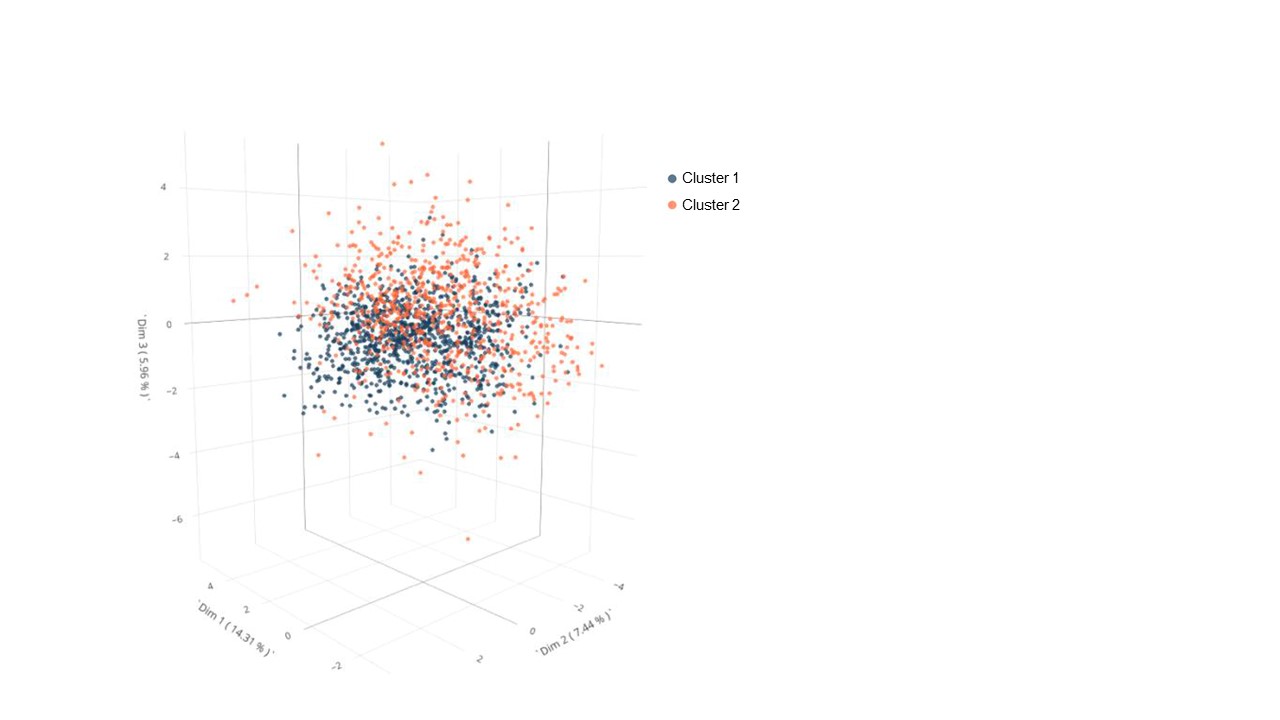
The map is a 3D representation of patients and their clusters (n = 1696). A point represents a patient, and its color represents the cluster assigned to this patient (cluster 1 in blue and cluster 2 in orange). The first three dimensions of MCA together explain 27.7% of the total variance.
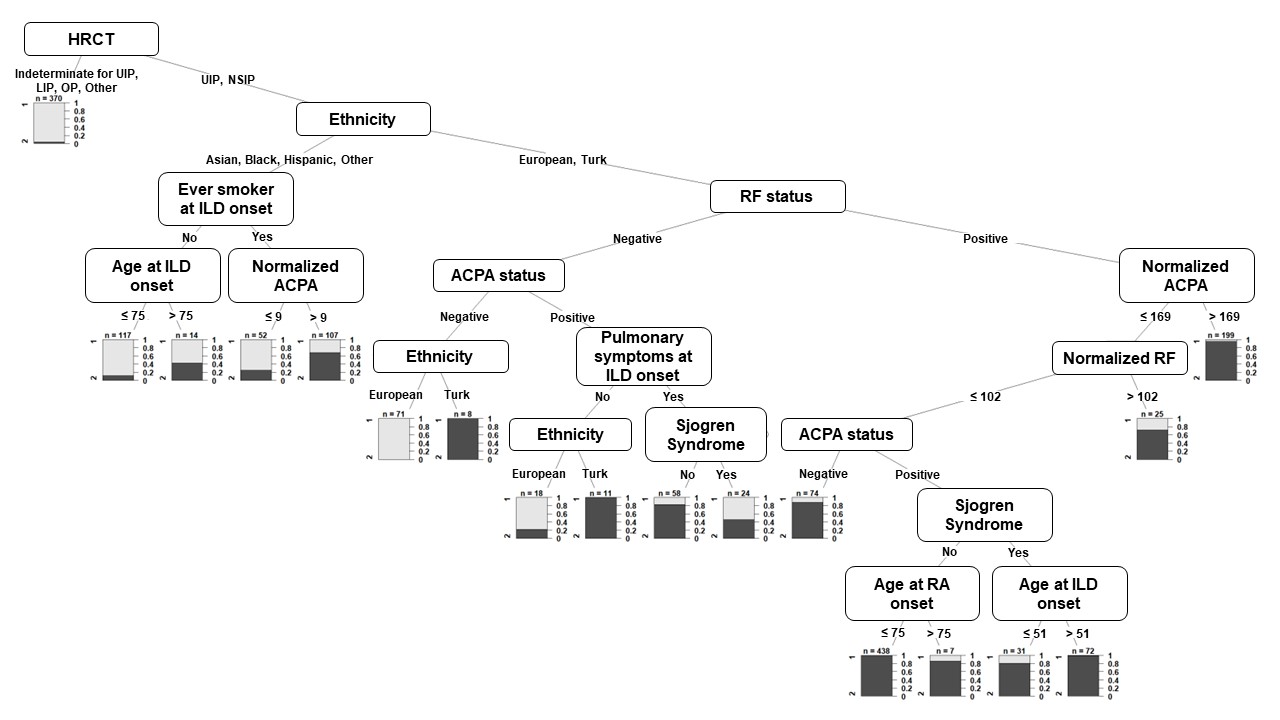
The tree is a set of paths. Each path is a sequence of conditions that lead to a decision (cluster 1 or cluster 2). The nodes present active variables that are important in the decision-making and the edges present conditions to be checked by a patient in order to classify him in one of the two clusters. The barplot (final node of each path) presents the two clusters (cluster 1 and cluster 2) on the left and the probability to be in cluster 1 on the right. ACPA: anti-citrullinated peptides antibodies; HRCT: high-resolution computed tomography; ILD: interstitial lung disease; LIP: lymphocytic interstitial pneumonia; NSIP: non-specific interstitial pneumonia; OP: organizing pneumonia; RF: rheumatoid factor; UIP: usual interstitial pneumonia
To cite this abstract in AMA style:
Juge P, Granger B, El Houari L, McDermott G, Doyle T, Kelly C, Koduri G, Vassallo R, Alarcon Calderon A, Kalyoncu U, Gonzalez A, Mena Vazquez N, Rojas M, Dos-Santos R, Retuerto-Guerrero M, Vadillo-Font C, VELA P, Fernandez-Nebro A, Escudero-Contreras A, Perez-Pampin E, Hyldgaard C, Froidure A, Durez P, Rojas Serrano J, van Moorsel C, Grutters J, Kawano-Dourado L, Lucas C, Jouneau S, Sanmarti R, Castellanos Moreira R, Antoniou K, Molina molina M, Solomon j, raia S, Gonzalez-Gay M, Atienza-Mateo B, Flouda S, Manali E, Dimitrios B, Papiris S, KARAGEORGAS T, Sebastiani M, Manfredi A, Duarte A, Castañeda S, Cavagna L, Crestani B, Sparks J, Dieudé P. Deciphering Rheumatoid Arthritis-associated Interstitial Lung Disease Phenotypes Using Unsupervised Hierarchical Clustering Analysis: Results from a Large Collaborative International Study [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/deciphering-rheumatoid-arthritis-associated-interstitial-lung-disease-phenotypes-using-unsupervised-hierarchical-clustering-analysis-results-from-a-large-collaborative-international-study/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/deciphering-rheumatoid-arthritis-associated-interstitial-lung-disease-phenotypes-using-unsupervised-hierarchical-clustering-analysis-results-from-a-large-collaborative-international-study/