Session Information
Session Type: Breakout Session
Session Time: 5:10PM-5:40PM
Background/Purpose: Clinical registries are typically envisioned to be representative of a target patient population and reflective of health care delivery practices for said population. Variation in clinical practices by different sites and concerns related to recruitment/retention can have profound implications for the validity of data collected and extent to which it may be impacted by selection bias. Thus, the objective of this study is to assess the role of patient- and site-level factors associated with research attrition in the Childhood Arthritis and Rheumatology Research Alliance (CARRA) Registry.
Methods: Patients enrolled in the CARRA Registry from 2015 to 2019 were eligible. The effects of patient (level 1) and site (level 2) factors on lost to follow-up were assessed using a 2-level logistic model, followed by empirical Bayes estimation to investigate cross-center variation. Sites classify patients as inactive if they are referred elsewhere, move to a non-CARRA site, transition to adult rheumatology, achieve remission, or are lost to follow-up. We defined our outcome of interest as patients lost to follow-up (= 1) versus all other patients (=0), who may be active or inactive due to other reasons. The empirical Bayes estimates are used to graphically illustrate variation in lost to follow-up rates between unadjusted and adjusted models (Figure 1).
Results: The final analytic sample contained 9,730 patients nested within 69 sites (Table 1). Most of the sample was female (n=6,481, 72%), White (n=6,403, 64%), and privately insured (n=5,559, 62%). Overall, 728 (7.5%) patients in the cohort were lost to follow-up. The intra-class correlation coefficient (ICC) from null model signified that 20.3% of the variance in lost to follow-up is at the registry site level. Percent of missed Registry visits (OR 1.09, 95% CI: 1.086, 1.12), non-Medicaid state insurance (OR 1.95, 95% CI: 1.15, 3.12), and an income between $25,000 and $49,999 (OR 1.52, 95% CI: 1.003, 2.31) were significantly associated with higher odds of lost to follow-up (Figure 2).
Conclusion: Significant variation in research participant lost to follow-up exists at the site level. Moreover, individual-level characteristics such as visit history, insurance status, and household socioeconomic status were associated with the likelihood of being lost to follow-up. This non-random attrition may also highlight concerns related to patient retention in clinical practice.
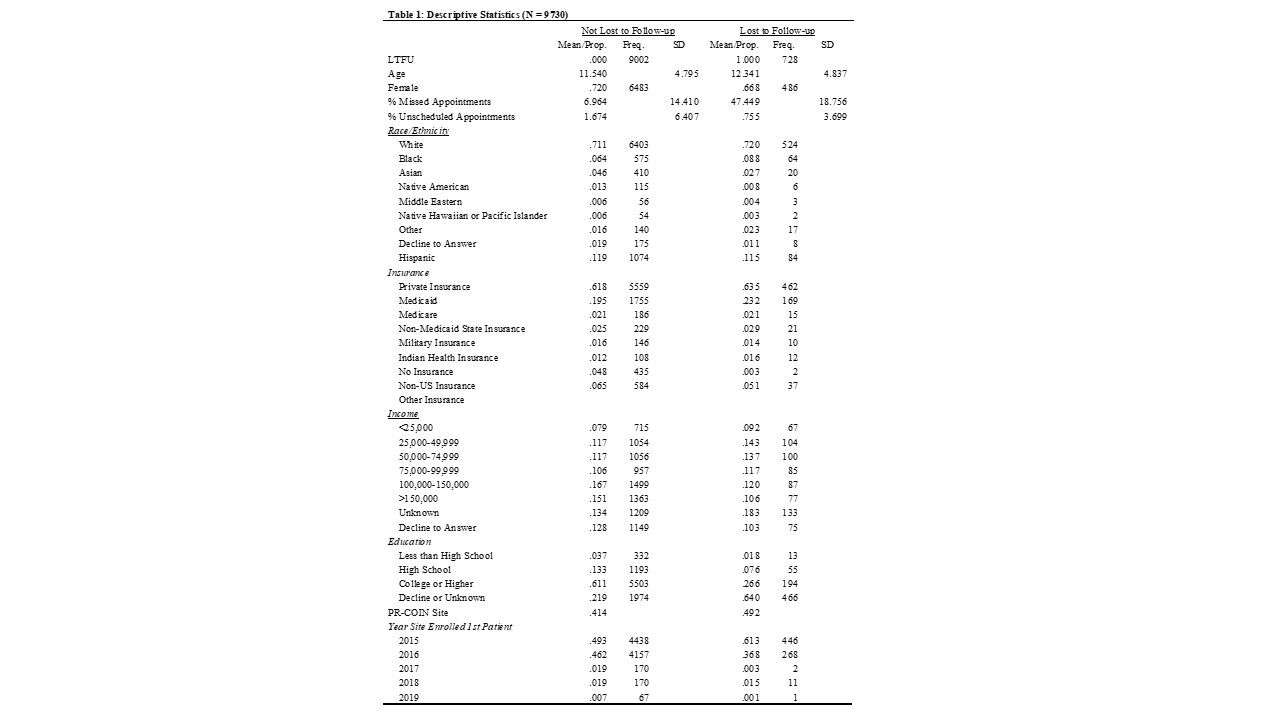 Table 1: Descriptive Statistics (N = 9730)
Table 1: Descriptive Statistics (N = 9730)
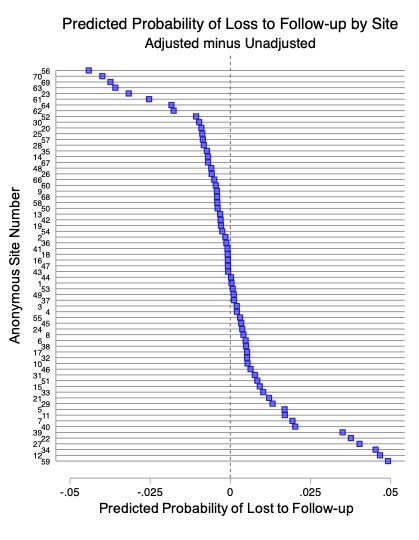 Figure 1: Site-level Variation. Sites with a negative difference (i.e., higher unadjusted predicted probability, to the left of zero) means controlling for patient- and site-level factors made their lost to follow-up look more favorable. Sites with a positive difference (i.e., higher adjusted predicted probability, to the right of zero) means controlling for patient- and site-level factors made their lost to follow-up look worse off.
Figure 1: Site-level Variation. Sites with a negative difference (i.e., higher unadjusted predicted probability, to the left of zero) means controlling for patient- and site-level factors made their lost to follow-up look more favorable. Sites with a positive difference (i.e., higher adjusted predicted probability, to the right of zero) means controlling for patient- and site-level factors made their lost to follow-up look worse off.
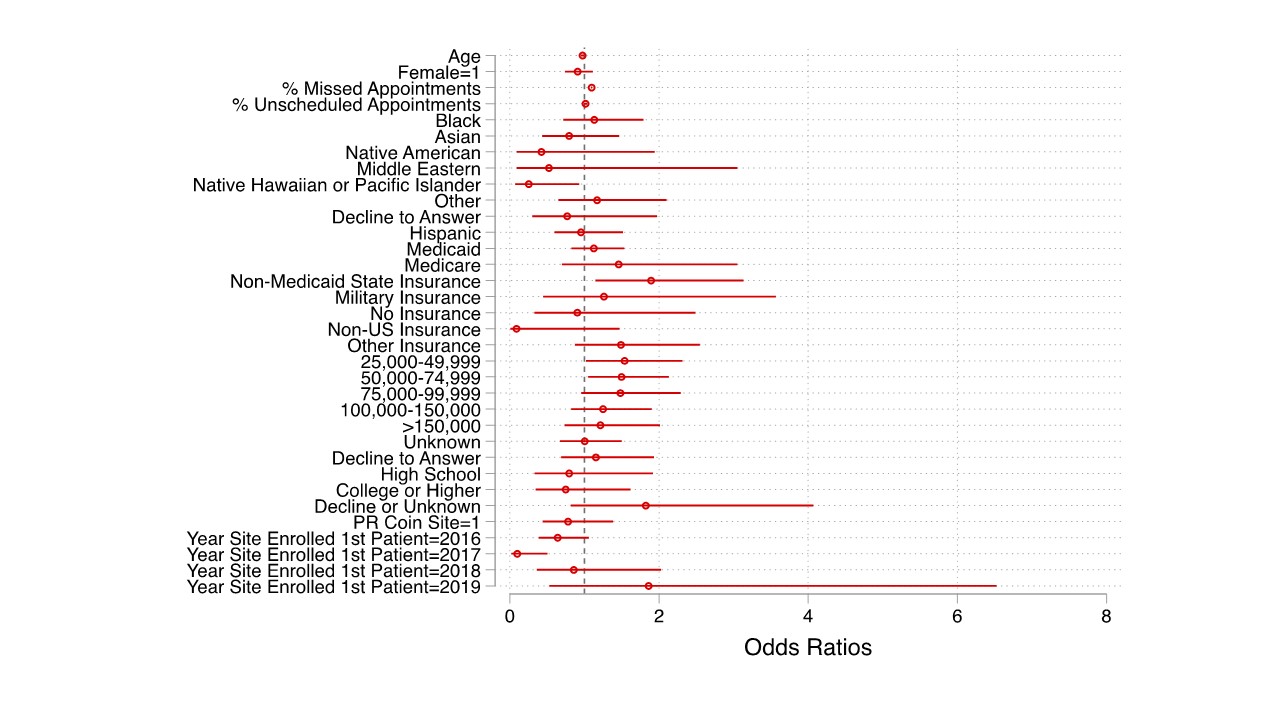 Figure 2: Multilevel Logistic Regression. Reference categories include: Male, White race, private insurance, less than high school, non-PR-COIN site, and site started CARRA enrollment in 2015.
Figure 2: Multilevel Logistic Regression. Reference categories include: Male, White race, private insurance, less than high school, non-PR-COIN site, and site started CARRA enrollment in 2015.
To cite this abstract in AMA style:
Aswani M, Huie L, Hearld K, Mannion M, Smitherman E. Patient- and Center-level Risk Factors for Research Lost to Follow-up Using the Childhood Arthritis and Rheumatology Research Alliance (CARRA) Registry [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 4). https://acrabstracts.org/abstract/patient-and-center-level-risk-factors-for-research-lost-to-follow-up-using-the-childhood-arthritis-and-rheumatology-research-alliance-carra-registry/. Accessed .« Back to 2023 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/patient-and-center-level-risk-factors-for-research-lost-to-follow-up-using-the-childhood-arthritis-and-rheumatology-research-alliance-carra-registry/