Session Information
Date: Sunday, November 8, 2020
Title: SLE – Diagnosis, Manifestations, & Outcomes Poster II: Comorbidities
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Cardiovascular events remain a major cause of morbidity and mortality in SLE. Accelerated atherosclerosis occurs in SLE and many other inflammatory diseases. In the general population both the Framingham Risk Score and the ACC/AHA Risk Equation combine stroke and myocardial infarction as the outcomes. The prospective SLE Cardiovascular Risk Equation took the same approach. The model found that traditional risk factors (age, sex, ethnicity, systolic blood pressure, total cholesterol, smoking, and diabetes mellitus) and SLE-specific risk factors (low C3 and lupus anticoagulant) were independent predictors of a later cardiovascular event (Lupus Sci Med. 2019;6:e000346). In this study, we took a different approach, and examined risk factors separately for myocardial infarction and for stroke.
Methods: SLE was defined by the revised ACR or SLICC classification criteria. Cardiovascular events were defined as myocardial infarction (MI) or stroke (ACC/AHA definition). In our cohort of 2,398 patients, 1,029 were African-American and 1,369 Caucasian. Nineteen were missing a SLE diagnosis date and 9 had missing data on events. There were 230 strokes and 116 myocardial infarctions.
Results: Table 1 shows the multivariate model of predictors of myocardial infarction and of stroke in SLE. Surprisingly, demographic variables such as age at diagnosis and African-American race were not risk factors. Male gender was a risk factor only for MI. Traditional cardiovascular risk factors were present for both outcomes, but overlapped only for hyperlipidemia and diabetes. Smoking was a risk factor only for MI. Hypertension was a risk factor only for stroke. The lupus-specific risk factors, low C3 and lupus anticoagulant, were only risk factors for stroke.
Conclusion: SLE is different from the general population in the predictive value of traditional cardiovascular risk factors for MI and stroke, with only hyperlipidemia and diabetes being risk factors for both. SLE-specific risk factors, low C3 and lupus anticoagulant, were important only for stroke. Attention to both traditional and SLE-specific risk factors remains paramount to lessen the cardiovascular morbidity of SLE. It is disappointing, however, that we do not have a clinically available SLE measure that predicts MI. We must still depend on non-invasive tests such as coronary CT or CT angiogram to identify patients early with atherosclerotic plaque.
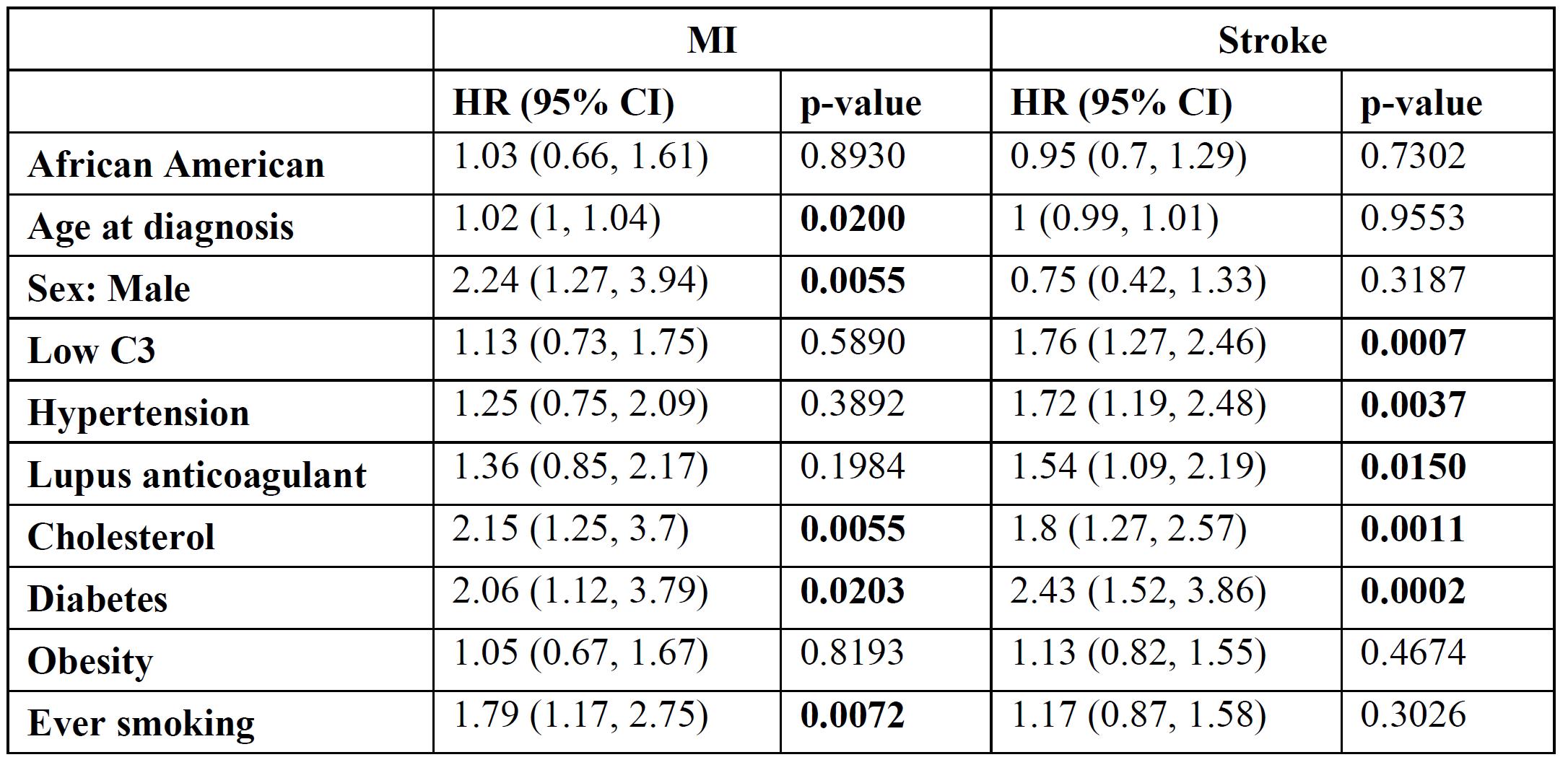 Relationships Between Predictors and MI/Stroke Based on a Multivariable Model
Relationships Between Predictors and MI/Stroke Based on a Multivariable Model
To cite this abstract in AMA style:
Petri M, Li J, Goldman D. Multivariate Risk Model Shows Different Risk Factors for Myocardial Infarction and Stroke in SLE [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/multivariate-risk-model-shows-different-risk-factors-for-myocardial-infarction-and-stroke-in-sle/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/multivariate-risk-model-shows-different-risk-factors-for-myocardial-infarction-and-stroke-in-sle/