Session Information
The 2020 Pediatric Rheumatology Symposium, originally scheduled for April 29 – May 2, was postponed due to COVID-19; therefore, abstracts were not presented as scheduled.
Date: Friday, May 1, 2020
Title: Plenary Abstracts Session 2
Session Type: Plenary Session II
Session Time: 2:30PM-3:00PM
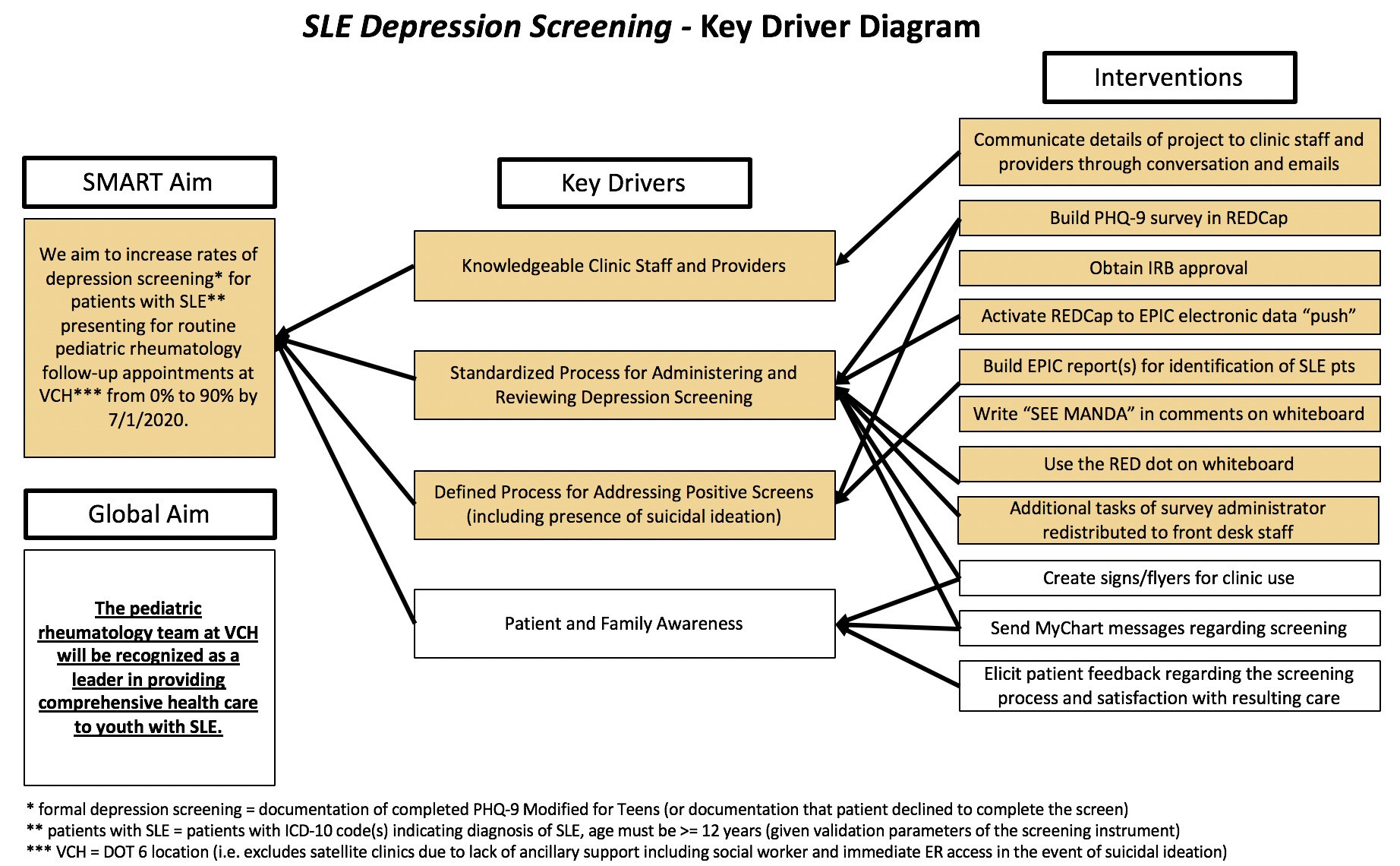
Background/Purpose: Depression is common among youth with SLE. Early identification and treatment of depression has the potential to improve health outcomes for youth with SLE. Pediatric rheumatologists are uniquely positioned to provide depression screening and intervention due to the frequency of patient encounters and ongoing therapeutic relationship with patients and families. The aim of this quality improvement project is to increase rates of standardized depression screening for patients with SLE presenting for follow-up appointments in our pediatric rheumatology clinic from 0% to 90% by July 1, 2020.
Methods: All patients with SLE (defined using specified ICD-10 codes) who are ≥ 12 years of age and seen for follow-up in our pediatric rheumatology clinic are included in the project. The Pediatric Health Questionnaire-9 (PHQ-9), a depression screen validated in both a general adolescent population and in patients with SLE, is administered via electronic tablet during the patient encounter and immediately uploaded to the EHR. Screens are automatically scored with treatment plans suggested for the provider based on severity of depression symptoms using the PHQ-9 standardized scoring and treatment algorithm. A multidisciplinary pediatric rheumatology clinic team (including resident, fellow, attending, social worker, case manager, nurse, and front desk staff) developed a key driver diagram to anchor potential project interventions (Figure 1). The team meets on a biweekly basis to plan and evaluate interventions using the structure of plan-do-study-act (PDSA) cycles. Statistical process control methods are used for data analysis.
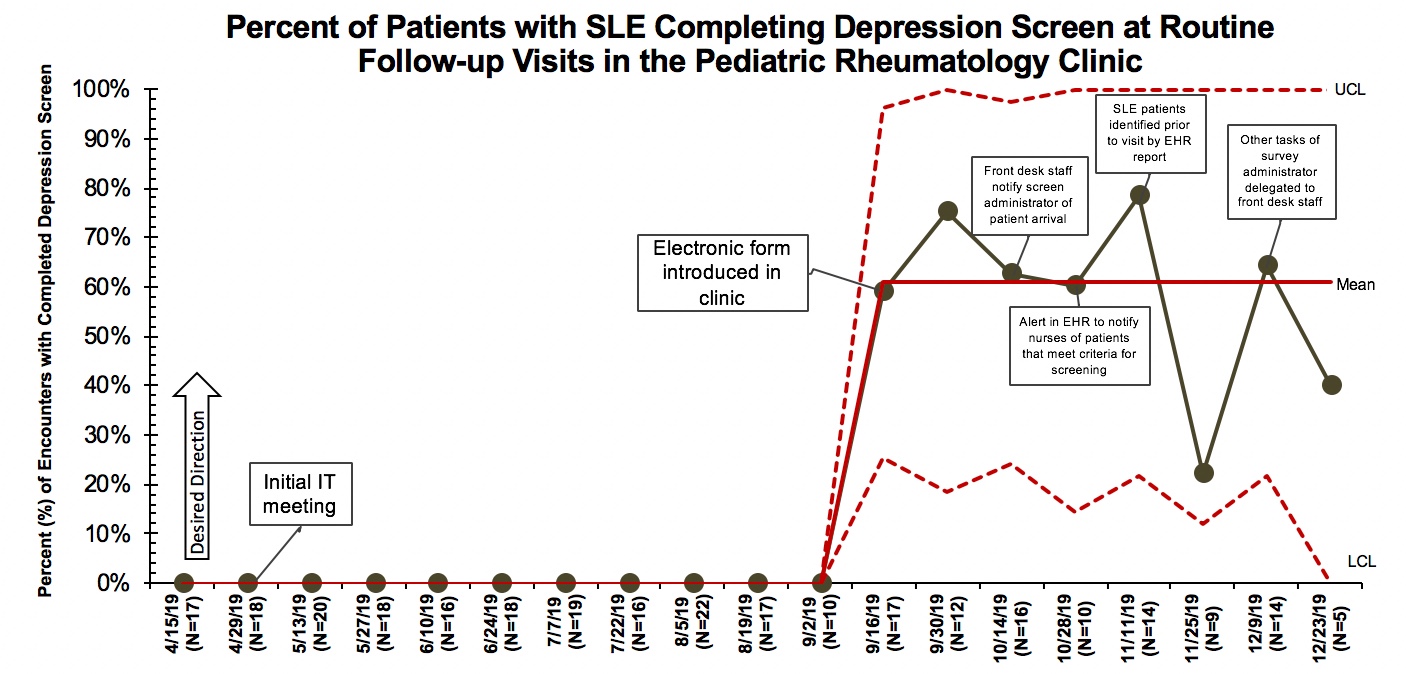
Results: The percentage of eligible patient encounters where depression screening was offered increased from 0% to 60.8% following implementation of the electronic PHQ-9 on September 16, 2019. This represents special cause variation as evidenced by a data shift (eight points above the mean line) on the control chart (Figure 2). Additional PDSA cycles are annotated on the control chart, but there are insufficient data points at this time to determine subsequent special cause. There were 9 encounters where the patient declined to complete the depression screen. Of the 50 completed depression screens, 26 (52.0%) were positive – 15 (57.7%) with mild, 9 (34.6%) with moderate, and 2 (7.7%) with severe depression symptoms. Suicidal ideation was identified in 5 patients. Appropriate interventions were documented including social work involvement, home safety plan, and psychiatry referral.
Conclusion: Rates of depression screening for youth with SLE significantly increased upon implementation of electronic PHQ-9 administration integrated with the EHR. Identification of patients with symptoms of depression and/or active suicidal ideation facilitated development of interventions that otherwise may not have been addressed during the patient encounter.Future PDSA cycles will focus on refining the current process of depression screening and incorporating insights from patients and families.
To cite this abstract in AMA style:
Newsome V, Dingle J, Mitchell M, Graham T, Davis A. Increasing Rates of Standardized Depression Screening in Youth with Systemic Lupus Erythematosus in a Pediatric Rheumatology Clinic [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 4). https://acrabstracts.org/abstract/increasing-rates-of-standardized-depression-screening-in-youth-with-systemic-lupus-erythematosus-in-a-pediatric-rheumatology-clinic/. Accessed .« Back to 2020 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/increasing-rates-of-standardized-depression-screening-in-youth-with-systemic-lupus-erythematosus-in-a-pediatric-rheumatology-clinic/