Session Information
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Osteoarthritis (OA) is the most common form of arthritis. Knee OA is often accompanied by a knee flexion contracture (FC), but the impact of FC on OA-related outcomes is not well-described. We evaluated whether the presence and/or severity of a knee FC were risk factors for increased OA incidence, clinical outcomes, radiographic progression and the need for and time to total knee arthroplasty (TKA).
Methods: The cohort design was based on 9-year longitudinal data from the osteoarthritis initiative (OAI) database. Participants (n=4,796) were divided into 3 sub-cohorts: at-risk of knee OA (n=3284), radiographically-established knee OA (n=1390), and low-risk controls (n=122). We categorized knee FCs as none, mild, moderate or severe, based on maximum knee extension at enrollment. The incidence of radiographic knee OA was based on those with Kellgren and Lawrence (KL) score < 2 at enrolment, but ≥2 on follow-up xray. Clinical outcomes (pain, stiffness and function) were evaluated using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scale. KL radiographic scores, and time to TKA were extracted from the database. Effect size of FC was evaluated using a linear mixed regression model.
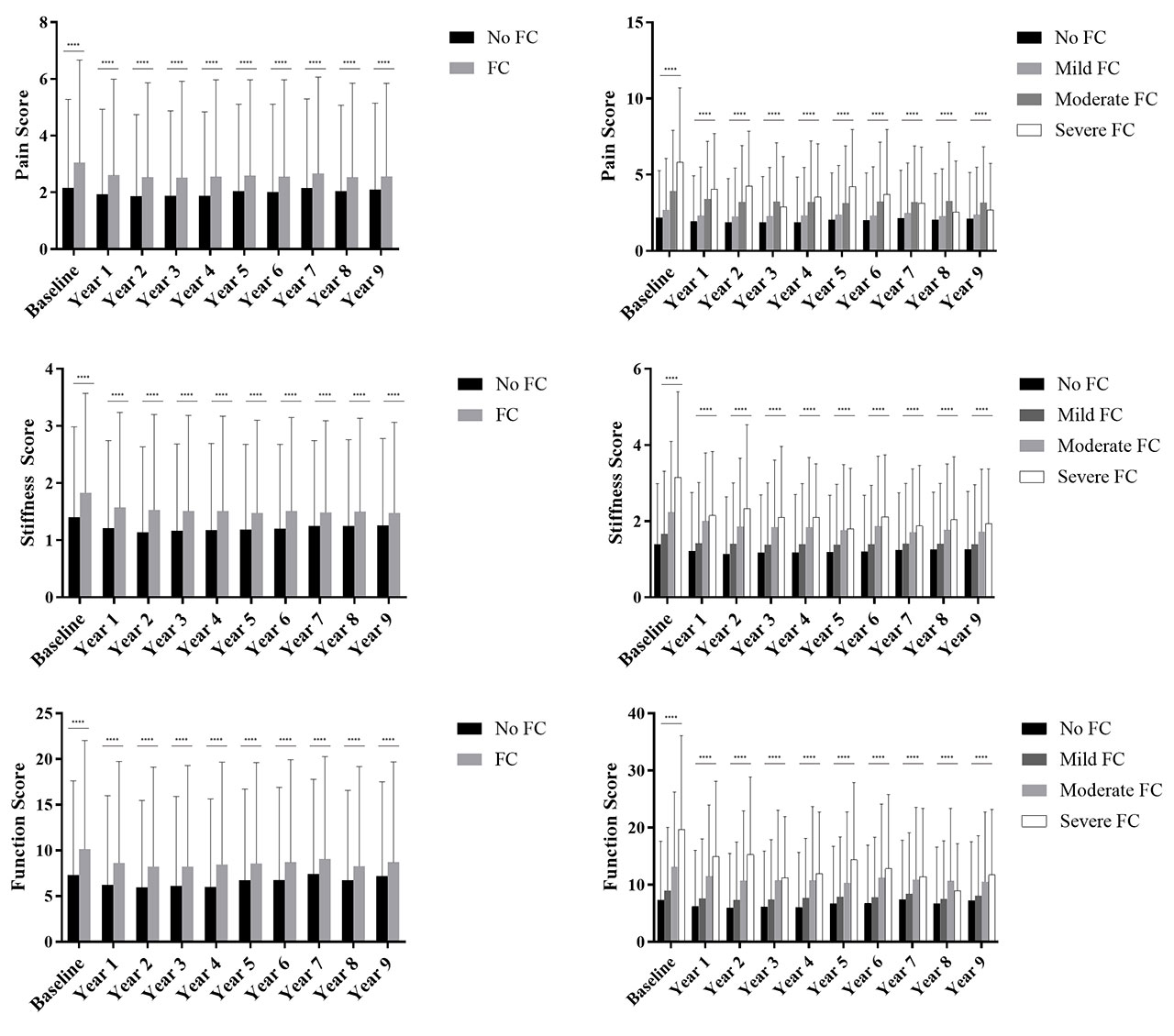
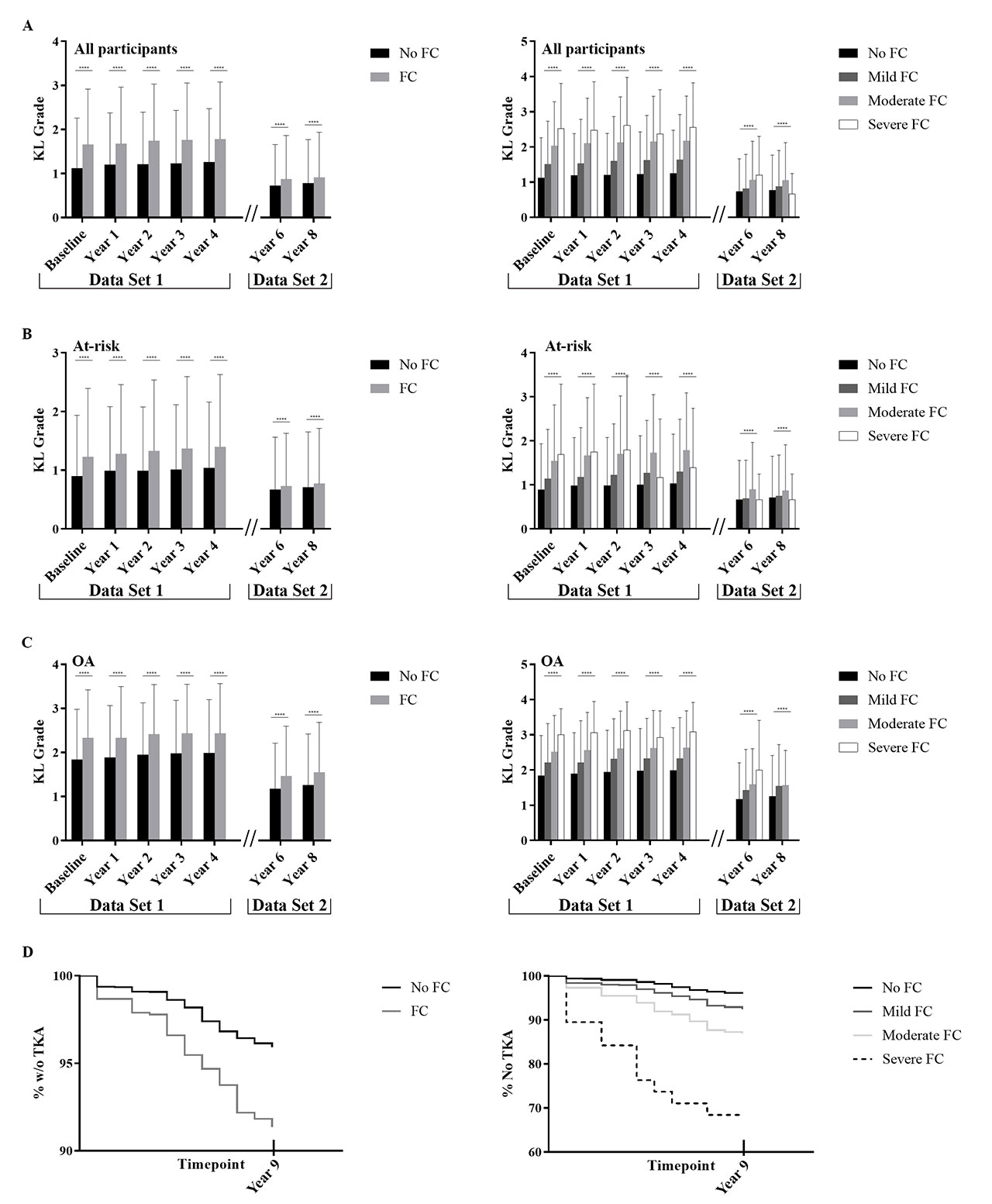
Results: Participants with knee FC without radiographic OA at enrolment did not have increased incidence of radiographic OA over the duration of data collection. The WOMAC pain, stiffness and function scores were worse in the FC group in a FC severity-dependent manner at nearly all timepoints (Figure 1). Effect estimates were significant for all 3 outcomes comparing FC vs no FC (0.17 [95% C.I. 0.12-0.22]) for pain, 0.12 [95% C.I. 0.09-0.14] for stiffness, 0.64 [95% C.I. 0.48-0.80] for function, all p< 0.001; Table 1). Those with knee FC had higher KL scores across all timepoints (effect size 0.38, p< 0.001, [95% C.I. 0.35-0.41]; Figure 2) with KL scores increasing with worsening FC severity (p< 0.001). Those with FC were more likely to undergo TKA (266/2819 or 9.4% with FC vs 246/5848 or 4.2% without FC, odds ratio 2.4 [95% C.I. 2.0-2.8], p< 0.001; Figure 2). After correcting for demographic variables, cohort, and baseline KL score, FC remained an independent predictor of TKA, in a severity dependent manner (Table 1). A FC was also a risk factor for having a TKA at an earlier timepoint (mean 279 days, p=0.024; Figure 2).
Conclusion: The presence of a knee FC at enrollment was a risk factor for worse clinical outcomes, radiographic progression, need for, and earlier time to TKA. Pain and OA-related structural changes may also lead to knee FC. Further research using MRI to define the anatomic/structural factors that contribute to FC and the link to OA progression are needed. Early and aggressive treatment of a knee FC may represent a treatment option for improving clinical outcomes and slowing OA progression in knee OA. Longitudinal evaluation of such treatment is needed.

To cite this abstract in AMA style:
Campbell T, McGonagle D. A Flexion Contracture Is a Risk Factor for Radiographic Progression and Earlier Need for Arthroplasty in Knee Osteoarthritis: Data from the Osteoarthritis Initiative [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/a-flexion-contracture-is-a-risk-factor-for-radiographic-progression-and-earlier-need-for-arthroplasty-in-knee-osteoarthritis-data-from-the-osteoarthritis-initiative/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-flexion-contracture-is-a-risk-factor-for-radiographic-progression-and-earlier-need-for-arthroplasty-in-knee-osteoarthritis-data-from-the-osteoarthritis-initiative/