Session Information
Date: Monday, November 11, 2019
Title: 4M117: RA – Treatments III: Cardiovascular Disease & Readmissions (1890–1895)
Session Type: ACR Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: Biologic disease-modifying antirheumatic drugs (bDMARDs) may decrease cardiovascular events (CVE) in Rheumatoid arthritis (RA). We here evaluated whether bDMARDs reduce long-term CVE risk in RA; we further explored whether potential benefits were rendered by altering the trajectory of coronary plaque progression or stability.
Methods: One hundred-fifty patients without CV disease underwent a baseline coronary computed tomography angiography (CCTA) and followed thereafter; 101 underwent repeat CCTA within 83±3.6 months. Coronary artery calcium (CAC) was quantified by the Agatston method. Segment involvement score (SIS) reported numbers of coronary segments with plaque; segment stenosis score (SSS) reflected the cumulative plaque stenosis. Plaque composition was defined as non-calcified (NCP), mixed or calcified. Lesions containing necrotic cores (low attenuation plaques-LAP) were deemed vulnerable. Cox proportional hazards regression models with time-varying covariates evaluated predictors of CVE. Robust logistic regression was used to assess plaque progression, and a generalized linear model with a Tweedie (Poisson-Gamma) error distribution for CAC change.
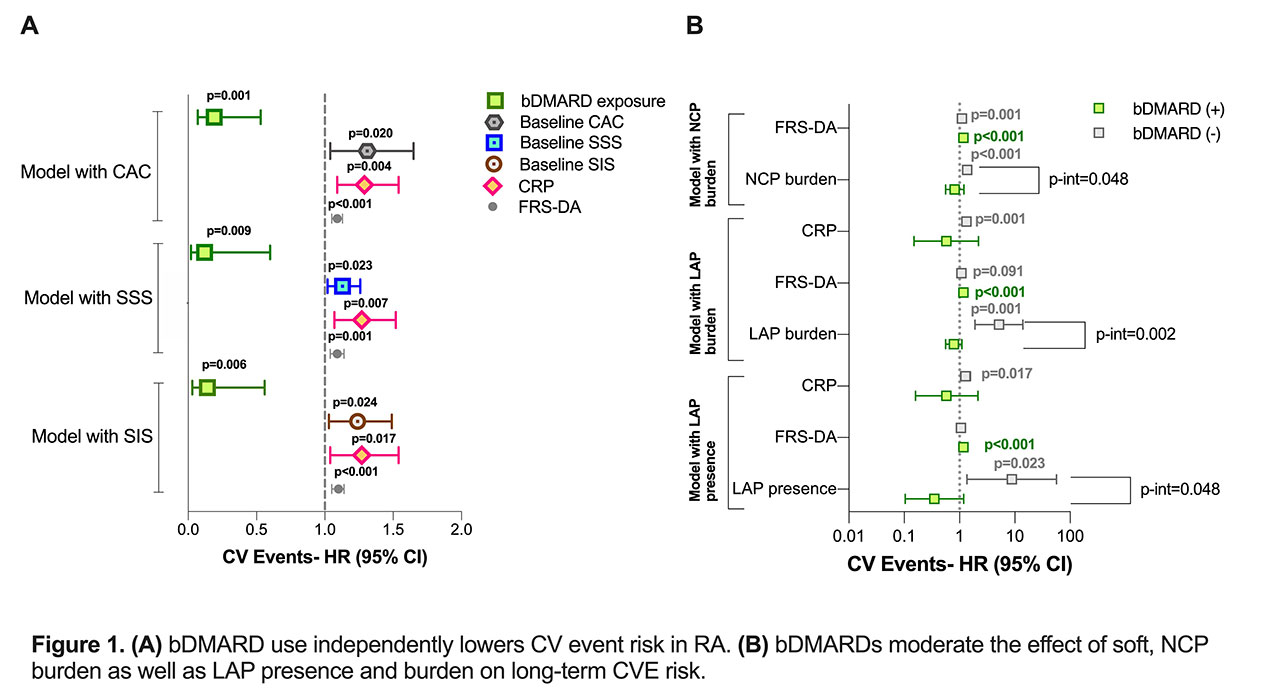
Results: Sixteen RA patients incurred 19 CVEs. Use of bDMARDs lowered CVE risk independently of cardiac scores, baseline atherosclerosis burden and time-varying CRP (Figure 1A, all p< 0.009). bDMARD use moderated the effect of baseline NCP burden on CVE risk (p-interaction=0.048); higher NCP load yielded higher risk only in bDMARD unexposed patients [HR=1.37 (1.16-1.61)], but not in exposed ones [HR=0.82 (0.56-1.20), Figure 1B]. Indeed, longer bDMARD use inhibited NCP progression independently of statin exposure, cumulative prednisone and methotrexate doses [OR=0.77 (0.61-0.98)]. Moreover, bDMARD use moderated the effect of baseline LAP presence and burden on CVE risk [p-interaction=0.048 and 0.002 respectively, Figure 1B]. LAP presence yielded an 8.8-fold [(1.36-56.80)] higher risk of CVE in patients not on bDMARDs but not in those on bDMARDs [HR=0.35 (0.10-1.19)]. Similarly, higher baseline LAP burden yielded greater CVE risk exclusively in patients not on bDMARDs [HR=5.16 (1.90-13.99)] but not in those receiving bDMARD [HR=0.79 (0.56-1.10)]. Longer bDMARD use reduced the likelihood of LAP presence on follow-up [OR=0.22 (0.07-0.69)] after adjustment for cardiac scores. Indeed, patients with LAP loss or lower LAP burden on follow-up had longer exposure to bDMARDs compared to those without [differences of 3.75 years (0.46- 7.04), p=0.028 and 6.08 years (3.02-9.13), p=0.001 respectively].
Conclusion: bDMARD use reduces CVE risk in RA, possibly by inhibiting non-calcified coronary plaque progression, remodeling and by stabilizing vulnerable plaques.
To cite this abstract in AMA style:
Karpouzas G, Ormseth S, Hernandez E, Budoff M. Biologics Prevent Cardiovascular Events in Rheumatoid Arthritis by Inhibiting Non-calcified Coronary Plaque Progression and Stabilizing Vulnerable Plaques [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/biologics-prevent-cardiovascular-events-in-rheumatoid-arthritis-by-inhibiting-non-calcified-coronary-plaque-progression-and-stabilizing-vulnerable-plaques/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/biologics-prevent-cardiovascular-events-in-rheumatoid-arthritis-by-inhibiting-non-calcified-coronary-plaque-progression-and-stabilizing-vulnerable-plaques/