Session Information
Date: Monday, November 11, 2019
Title: Pediatric Rheumatology – ePoster II: SLE, Juvenile Dermatomyositis, & Scleroderma
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: The traditional 1997 ACR SLE classification criteria classify a patient as having SLE if 4 of the 11 criteria have been met over time. In comparison, the 2018 ACR/EULAR SLE classification criteria uses a point system (2018-SLE-Score) for 22 clinical and immunologic domains (range:0-51; threshold score for SLE presence:10 points including an antinuclear antibody (ANA) titer of at least 1:80 on HEp-2 cells or an equivalent positive test). We investigated the difference of classifying patients with childhood-onset SLE (cSLE) when using the 2018 vs. 1997 SLE criteria. Further, we explored the association between the 2018 Criteria and disease activity in cSLE.
Methods: We reviewed the electronic medical record of ALL patients treated at a tertiary referral center carrying a diagnosis of cSLE, undifferentiated (UCTD) or mixed connective tissue disease (MCTD) from 2008 – 2018, as per the assessment of the treating pediatric rheumatologist. Patient data were reviewed starting from the initial encounter at the medical center, with external data reviewed if available. Disease activity as measured by the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) score was recorded within 1 month of diagnosis, and the most recent SLICC damage index (SDI) score was collected. SLEDAI and SDI scores were compared with the 2018-SLE-Score at initial diagnosis, and the sensitivity of 1997 ACR criteria and 2018 ACR criteria was compared to the current diagnosis of the patient’s pediatric rheumatologist.
Results: Our study consisted of 119 patients diagnosed with cSLE, UCTD, or MCTD: 87 (73.1%) were female with an average age at diagnosis of 14.56 years. These patients were predominantly white 68 (57.1%), black 36 (30.3%), and non-Hispanic 115 (96.6%; see Table 1). Of this cohort, the number of cSLE patients that were classified earlier using the 2018 criteria as compared to the 1997 SLE criteria was 9 out of 109 (8.3%) (See Table 2). The number of UCTD patients that were reclassified as SLE according to the 2018 criteria was 11 out of 33 (33.33%), and the number of MCTD that were reclassified was 4 out of 5 (80%). Our study found that there was neutral correlation between the SDI score and the 2018 SLE Score with a correlation coefficient= 0.28 and a median score of 22 that is associated with a patient SDI score > 1. The median 2018-SLE-Score that was associated with SLEDAI scores ≥ 6 during the first month post diagnosis was 16.5. 2018-SLE-Score and SLEDAI scores were moderately associated (r = 0.631; p= .000946). The sensitivity of the 1997 ACR criteria for our cohort was 83.78% and the 2018 ACR criteria was 88.29%. The 2018 ACR criteria were more sensitive but also produced more false positives (type I error; see Table 3). The median 2018-SLE-score of the 5 false positives was 10.8, close to the lower threshold for SLE presence.
Conclusion: Patients were found to be diagnosed earlier with cSLE using the 2018 ACR criteria among those carrying a current diagnosis of UCTD or MCTD . The 2018 ACR disease criteria proved to be more sensitive in detecting cSLE in our patient population than the 1997 ACR disease criteria. In addition, our study revealed that the 2018 criteria score did not correlate with patient disease damage as indicated by the recent SDI score.

Table 1
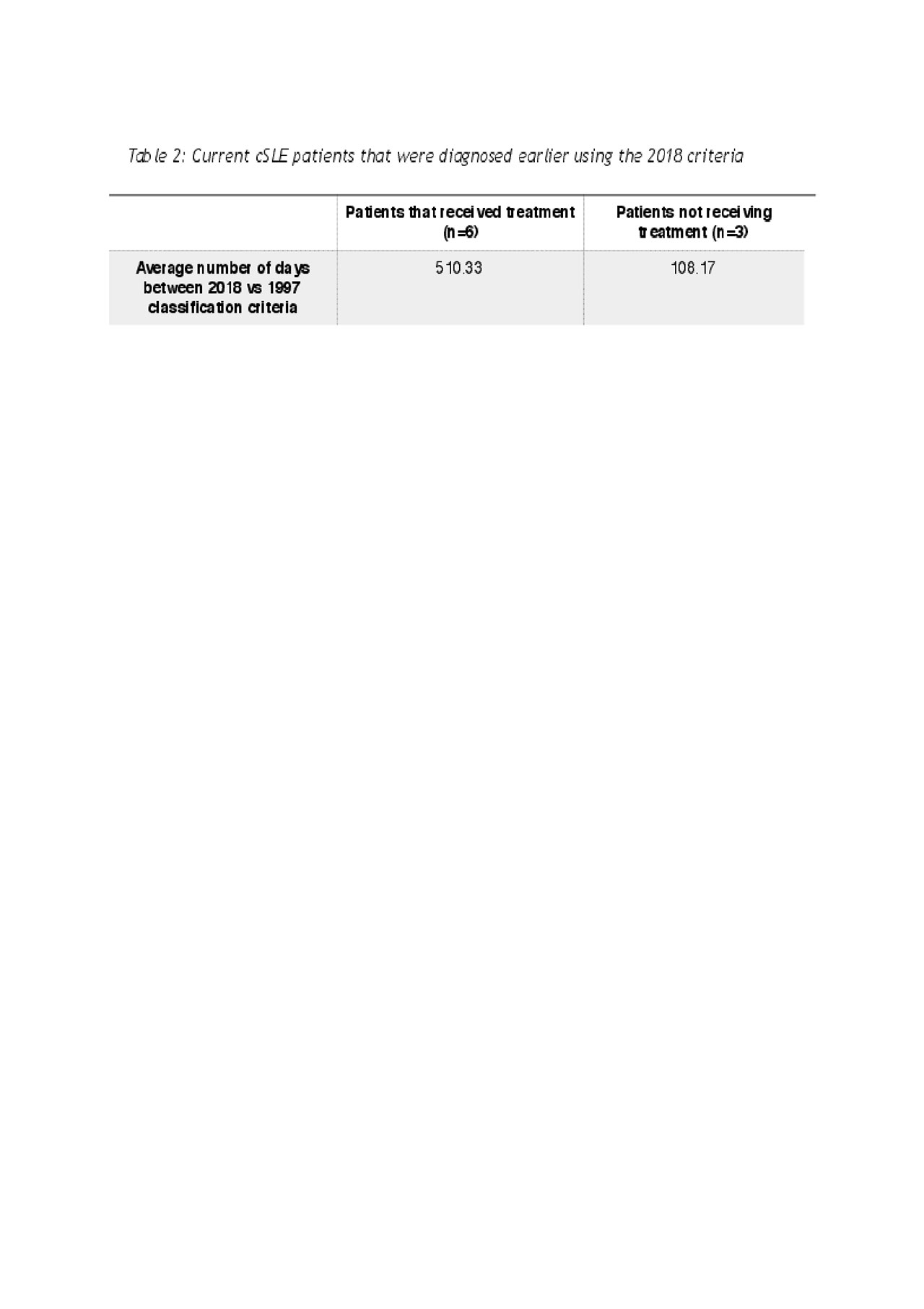
Table 2
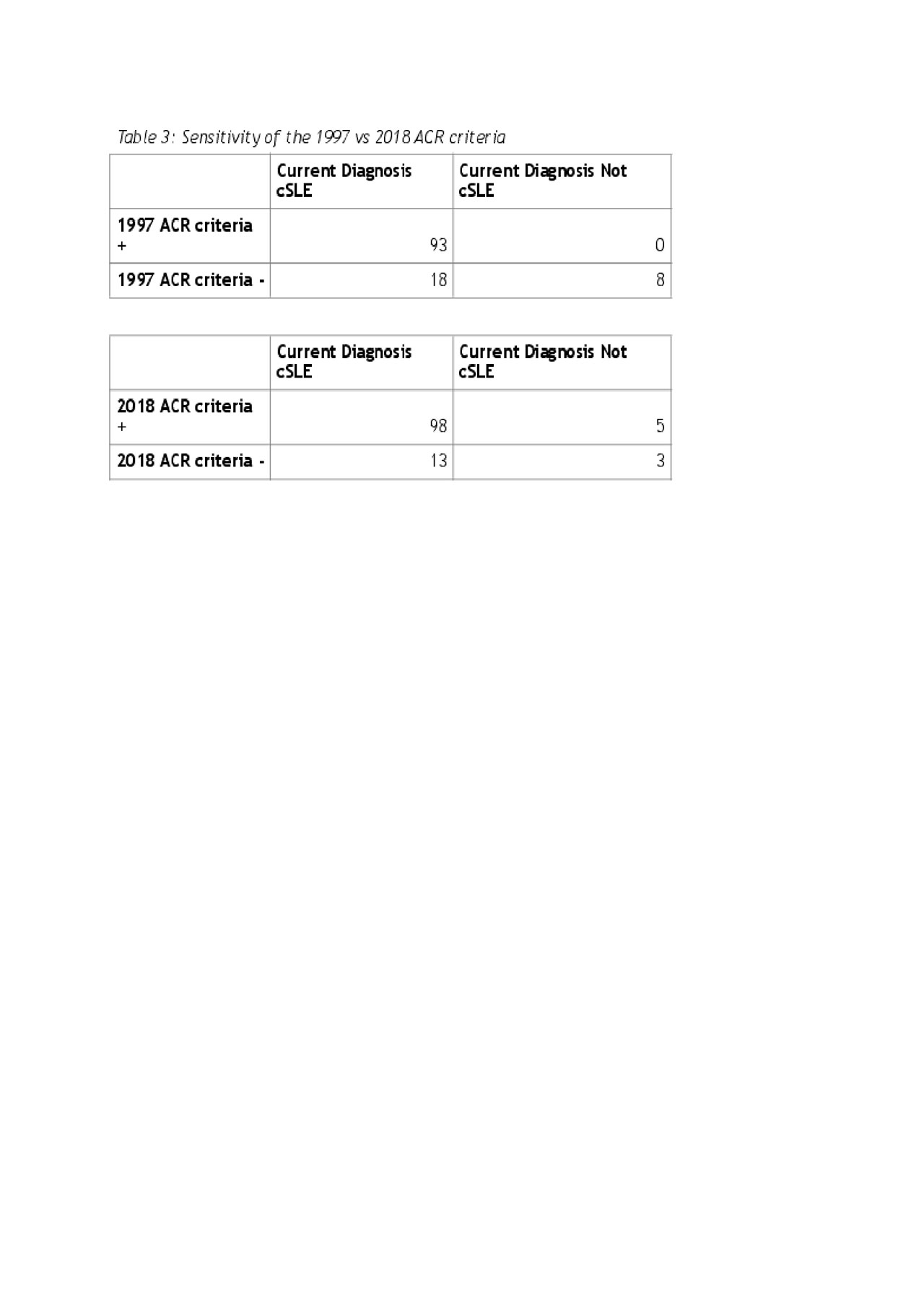
Table 3
To cite this abstract in AMA style:
Strahle C, Merritt A, Niu X, Mathur A, Watts A, Brunner H. Evaluating the New 2018 ACR/EULAR SLE Classification in Pediatric Patients [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/evaluating-the-new-2018-acr-eular-sle-classification-in-pediatric-patients/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/evaluating-the-new-2018-acr-eular-sle-classification-in-pediatric-patients/