Session Information
Date: Sunday, November 13, 2016
Title: Vasculitis - Poster I: Large Vessel Vasculitis and Polymyalgia Rheumatica
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: FDG-PET may have a role in diagnosing and monitoring disease activity in large vessel vasculitis (LVV). Studies that assess the diagnostic accuracy of PET in LVV often use patients with cancer as a comparator group. There are limited data regarding use of serial FDG-PET imaging to monitor disease activity, and most assessments are performed during periods of clinically apparent disease. This study assesses the diagnostic performance of PET to differentiate LVV from mimics of vasculitis, examines the role of PET as a measure of disease activity, and determines the clinical characteristics associated with abnormal vascular FDG uptake.
Methods: 42 patients with LVV and 50 comparators (15 with systemic inflammation, 35 with atherosclerosis) were recruited in this prospective, observational cohort. Patients with LVV underwent FDG-PET every 6 months. Clinical and imaging assessments were performed blinded to each other and to levels of acute phase reactants. FDG-PET/CT was performed with 120 min uptake time (256 matrix, 3 mm slice). Active vasculitis on PET was defined by agreement of two nuclear medicine experts and inter-rater agreement was assessed by the kappa statistic. Multivariable regression, adjusted for repeated measures, assessed associations between active vasculitis on PET and clinical characteristics.
Results: 125 FDG-PET scans were performed in 92 patients: giant cell arteritis (n=22; mean age 68.4±9.4 years; disease duration 2.4±2.5 years), Takayasu arteritis (n=20, mean age 34.9±11.2 years; disease duration 13.4±11 years) and comparators (n=50, mean age 53.6±15.3 years). Inter-rater agreement was high (kappa = 0.84). In patients with LVV with clinically active disease, the performance characteristics of PET as a diagnostic test were good (sensitivity 90%; specificity 86%); however, 17% of patients with atherosclerosis had PET scan findings indistinguishable from active vasculitis. 26 of 45 PET scans (58%) performed in patients with LVV during apparent clinical remission suggested ongoing active vasculitis. Clinically apparent active disease and shorter disease duration were significantly associated with an abnormal PET scan. There was no association between levels of acute phase reactants and PET abnormalities; treatment with immunomodulating medications had a non-statistically significant protective effect (Table).
Conclusion: FDG-PET is useful to distinguish active LVV from mimics of vasculitis, but patients with atherosclerosis can have PET scan findings that closely resemble LVV. The majority of patients with LVV have abnormal PET scans while in clinical remission. An inverse association between disease duration and PET abnormalities suggests that scan abnormalities observed during clinical remission are not due to accrued vascular damage. FDG-PET may be an important modality to detect and monitor subclinical inflammation in LVV. 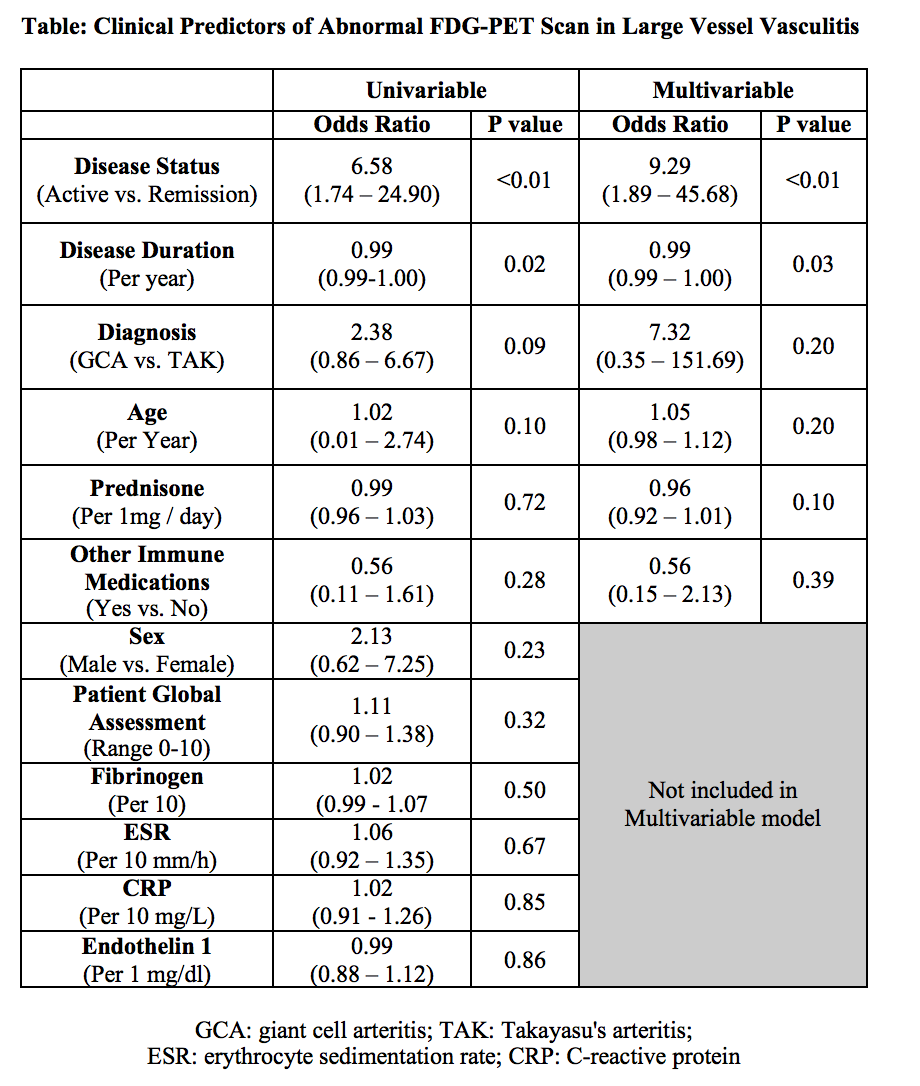
To cite this abstract in AMA style:
Alehashemi S, Ahlman M, Civelek AC, Novakovich E, Malayeri A, Merkel PA, Cupps T, Bluemke D, Grayson PC. Utility of 18f FDG Positron Emission Tomography (PET) As a Diagnostic Test and Marker of Disease Activity in Large Vessel Vasculitis [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/utility-of-18f-fdg-positron-emission-tomography-pet-as-a-diagnostic-test-and-marker-of-disease-activity-in-large-vessel-vasculitis/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/utility-of-18f-fdg-positron-emission-tomography-pet-as-a-diagnostic-test-and-marker-of-disease-activity-in-large-vessel-vasculitis/