Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Different definitions of clinically inactive disease (CID) for JIA have recently been shown to identify different groups of children. It is unclear whether long-term outcomes, such as low disability, differ between children who, early in disease, have no objective inflammatory signs (CID on Wallace’s preliminary criteria) versus those who also have good global wellbeing (CID on clinical Juvenile Arthritis Disease Activity Score (cJADAS)). It is also unclear whether achieving CID is more beneficial to long-term outcomes than achieving minimal disease activity (MDA). This study assessed whether functional outcome within five years, measured by the Childhood Health Assessment Questionnaire (CHAQ), differs according to disease activity state at one year following presentation in children with JIA.
Methods: Children recruited to the Childhood Arthritis Prospective Study (CAPS), a multicentre UK inception cohort, prior to 1st January 2011 and with a physician’s diagnosis of JIA (limited to oligoarticular, RF negative or positive polyarticular subtypes) were selected. At one year following presentation, children were categorised into three disease states: i) CID using both Wallace’s preliminary criteria and cJADAS, ii) CID using Wallace’s preliminary criteria only and iii) No CID. In addition, children were assessed for MDA using the cJADAS. CHAQ scores were compared between each disease state group via univariate and multivariate zero-inflated negative binomial regressions with robust clustering at the patient level. Multivariate models adjusted for age and symptom duration at presentation, gender and ILAR subtype. Multiple imputation accounted for missing data.
Results: Of 832 children, 70% were female and the most common subtype was oligoarthritis (68%), followed by RF-negative (27%) and RF-positive polyarthritis (5%). At one year, 22% had achieved CID according to Wallace’s preliminary criteria and cJADAS, 7% according to only Wallace’s preliminary criteria and 56% to neither. Compared with those who had not achieved CID, children who had achieved CID on both tools at one year had 21% lower CHAQ scores (95% CI 10, 31%) and double the odds of zero disability (95% CI 1.5, 2.6) within the first five years. However, those who had achieved CID only on Wallace’s preliminary criteria had similar CHAQ scores to the no CID group. There was no difference in functional ability between children who had achieved MDA or CID using JADAS at one year, with both achieving 27% lower CHAQ and having three times the odds of zero disability compared with children not in these states (Table 1).
Conclusion: Better long-term functional ability was only observed to increase when both objective measures of inflammation and subjective measures of the global picture of disease were taken into account. MDA may be an equally valid, but more feasible, treatment target to CID in patients with JIA. 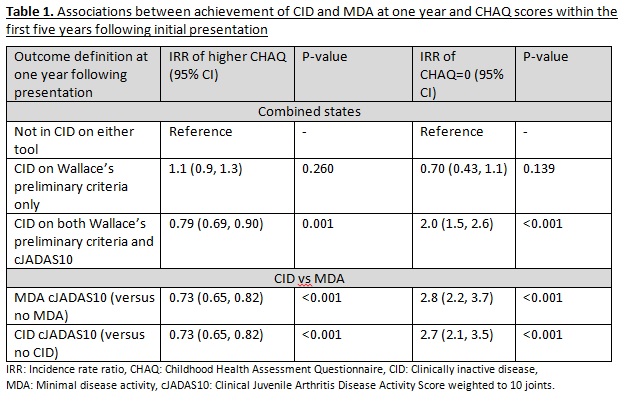
To cite this abstract in AMA style:
J.W.Shoop S, Verstappen SMM, E. McDonagh J, Thomson W, Hyrich KL. The Influence of Early Achievement of “Clinically Inactive Disease” or “Minimal Disease Activity” on Long-Term Disability Outcomes in JIA [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/the-influence-of-early-achievement-of-clinically-inactive-disease-or-minimal-disease-activity-on-long-term-disability-outcomes-in-jia/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-influence-of-early-achievement-of-clinically-inactive-disease-or-minimal-disease-activity-on-long-term-disability-outcomes-in-jia/