Session Information
Date: Sunday, November 8, 2015
Title: Epidemiology and Public Health I: RA Comorbidities and Mortality
Session Type: ACR Concurrent Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: Studies among unselected patients with rheumatoid arthritis (RA) suggest
increased risks of both ischemic and non-ischemic heart failure (HF). Since the
risk of these two subtypes of HF have not been assessed simultaneously within the
same cohort of RA-subjects, let alone in relation to time before/after RA
diagnosis, the objectives of this study were to assess the relative risk (RR) of
HF by subtype and to determine RR in different time periods since RA onset, in
one and the same cohort.
Methods: We
identified all subjects above 18 years of age with incident RA within the Swedish
Rheumatology Quality register (SRQ). All RA subjects were matched with up
to 10 general population comparator subjects based on sex, age, and area of
residency. The date of diagnosis was defined as the index-date; comparators
received the same index-date as their corresponding RA patient. Ischemic HF was
defined on the basis of ICD codes from linkage to the nationwide Patient
Register as i) a diagnosis of any HF after a diagnosis of IHD or ii) a main
diagnosis of ischemic HF, and was investigated in all subjects free of any HF
at the index-date. Non-ischemic HF was defined as a diagnosis of HF in individuals
without prior IHD-diagnosis, and was assessed in all subjects free of HF at
index date and free of IHD by the date of the HF outcome. Study subjects were
followed from the index-date until Dec 31st 2012 and censored at
death, first migration, IHD and ischemic HF (when the outcome was non-ischemic
HF), and HF (without antedating IHD) when the outcome was ischemic HF. Crude
rates were calculated and presented as numbers of events per 1,000 person-years.
As a measure of the RR of HF, hazard ratios (HRs) were obtained using cox
regression models, and odds ratios were calculated using logistic regression as
a measure of RR prior to the index-date.
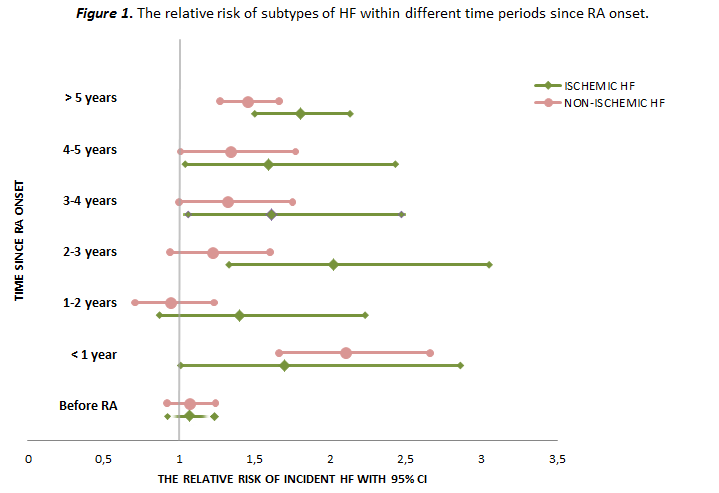
Results: In
total, 15,572 RA subjects and 132,018 comparators were free of HF at the
index-date, and 14,581 RA subjects and 12,4406 comparators were free of both HF
and/or IHD at index date. During follow-up 566 (6.7/1000 person-years) RA
subjects and 3413 (4.5/1000 person-years) comparators developed a first non-ischemic
HF, corresponding to a 40% risk increase for the RA subjects (HR 1.43 [95% CI
1.30-1.56]). 259 (2.9/1000 person years) RA subjects and 1,254 (1.6/1000
person-years) comparators developed ischemic HF during the follow-up,
translating into an 80% risk increase for the RA subjects (HR 1.77 [95% CI
1.55-2.03]). For both HF subtypes, stratification by sex did not reveal any
differences between sexes, HRs were higher for RF-positive compared to
RF-negative patients. For both subtypes, the RR went from null prior to the
index-date to increased risks soon after start of follow-up.
Conclusion: RA
is associated with an increased risk of both ischemic and non-ischemic HF. Differences
in when and how, in relation to RA onset the risks develop may suggest that several
mechanisms mediate HF risks in RA.
To cite this abstract in AMA style:
Mantel , Holmqvist M, Andersson D, Lund L, Askling J. Patients with Rheumatoid Arthritis Are at Increased Risk of Both Ischemic and Non-Ischemic Heart Failure [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/patients-with-rheumatoid-arthritis-are-at-increased-risk-of-both-ischemic-and-non-ischemic-heart-failure/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/patients-with-rheumatoid-arthritis-are-at-increased-risk-of-both-ischemic-and-non-ischemic-heart-failure/