Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Studies describing seasonal variations
in acute gouty arthritis note a seasonal trend, but disagree on timing, with
most showing a peak in spring months while others showing peaks later in the
year. The peak serum uric acid (SUA) levels however, have been found to be in
the summer months. This disparity has led to the hypothesis that the flares
might be related to factors other than high SUA levels. Various theories on the
effect of weather and immune system changes on the chronobiology of the
equilibrium and precipitation of monosodium urate crystals have been proposed.
We aimed to shed light on this question by examining the seasonal variation in
the incidence of acute gouty arthritis in the US using a large inpatient
database.
Methods: We used the Nationwide Inpatient Sample (NIS)
database to identify patients aged ≥ 18 years with primary diagnosis of acute gouty arthritis
ICD-9-CM code 274.01 from 2009-2011 during hospitalization. We used the Edwards’
recognition and estimation of cyclic trend method to study the seasonal
variation of the incidence of acute gout and Z-test to compare the seasonal
incidences.
Results: A total of 28,172 hospitalizations with primary
diagnosis of acute gouty arthritis were reported in during the period. The peak
incidence of acute gout was seen in November (peak/low ratio 1.34, 95% CI
1.29-1.38, p<0.05) (Figure 1). The highest number of hospitalizations was
observed in autumn months while the lowest incidence was observed in spring
(28.12% vs. 23.13%, p<0.001).
Conclusion: Unlike previous studies, our analysis found the
peak incidence of acute gout in the fall with its peak in the month of
November. Various environmental (temperature, humidity, diet, physical
activity) and biochemical factors (low cortisol levels, high absolute
neutrophil counts and plasminogen activator inhibitor-1) have been implicated
for the seasonal variation. There have been conflicting data on the correlation
of the incidence of acute gouty arthritis with environmental factors such as
temperature or humidity. Dehydration during summer months has been postulated
to precipitate crystal formation. In contrast, lower temperatures have also
been reported to precipitate monosodium urate crystals in vitro, however
cooling the joints with ice has been found to improve recovery. Whether our
findings are reflective of purine and alcohol intake over the US holidays in
November and December is a hypothesis that requires further testing. Further
studies are required to verify whether seasonal, hormonal, dietary or
immunological changes and acute-phase reactants have a role in the pathogenesis
of acute flares. The control of these factors could potentially lead to better
management of patients with gout who are at risk of acute attacks and perhaps
prevent these attacks.
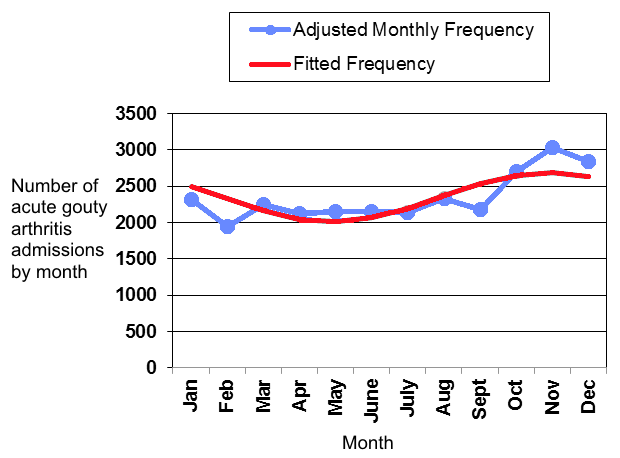
Figure 1. Graph showing seasonal
trend for acute gouty arthritis admissions, 2009-2011
To cite this abstract in AMA style:
Karmacharya P, Pathak R, Aryal M, Giri S, Donato A. Seasonal Variation in Acute Gouty Arthritis: Data from Nationwide Inpatient Sample [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/seasonal-variation-in-acute-gouty-arthritis-data-from-nationwide-inpatient-sample/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/seasonal-variation-in-acute-gouty-arthritis-data-from-nationwide-inpatient-sample/