Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Previous reports on a window of opportunity (WOO) in rheumatoid arthritis (RA) may be related to the use of slow acting csDMARDs. We investigated whether onset of action of therapy might influence whether there is a WOO or whether ‘earlier is better’. Therefore we aimed to investigate the association between symptom duration at treatment onset and the achievement of sustained drug free remission (sDFR) in early RA patients initiating therapy including fast acting prednisone or infliximab, compared to patients initiating csDMARD monotherapy.
Methods: We analysed the shape (non-linear or linear) of the association between symptom duration and achievement of sDFR (DAS<1.6 and no DMARDs for ≥1 year) in 3 cohorts: BeSt, IMPROVED and METEOR. Patients had arthritis symptoms <2 years. In BeSt, RA-patients (1987 criteria) were randomised to 4 targeted treatment strategies aimed at DAS≤2.4: arm 1 and 2 initiated csDMARD monotherapy, arm 3 csDMARDs and tapered high dose prednisone and arm 4 csDMARD and infliximab. In IMPROVED RA patients (2010 criteria) were treated with csDMARD and tapered high dose prednisone. Subsequent treatment adjustments aimed at DFR. METEOR is an international observational cohort including daily practice data from RA patients with a diagnosis and treatment according to the rheumatologist. We selected patients who initiated csDMARD monotherapy or a combination of csDMARD with prednisone or anti-TNF and at least 1.5 year follow-up.
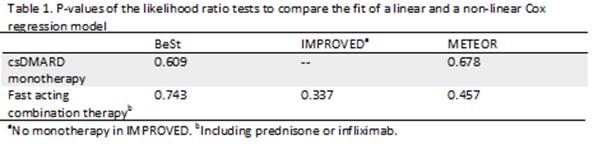
We performed Cox regression with as outcome sDFR and as predictor symptom duration and used likelihood ratio tests to compare the fit of a linear model and a model with inclusion of natural cubic spline functions (resulting in a hyperbola).
Results: In BeSt (n=469), IMPROVED (n=421) and METEOR (n=1268) 54, 110 and 10 patients who initiated fast acting combination therapy, and 53 in BeSt and 15 in METEOR who initiated csDMARD monotherapy achieved sDFR. A non-linear model did not show a better fit for the data than a linear model (table 1). Thus, we did not find a curved relationship between time of treatment initiation and achieving sDFR. The best fit models indicate that the earlier treatment is started, the higher the likelihood of achieving sDFR (figure 1).
Conclusion: Our data suggest that there is no evidence for a WOO in early RA in 3 cohorts. This was not related to use of fast acting combination therapy instead of slow acting monotherapy nor was it dependent on strict treat-to-target in clinical trials. Instead, our data reaffirm that earlier is better when treating RA.

To cite this abstract in AMA style:
Bergstra SA, van der Pol JA, Riyazi N, Goekoop-Ruiterman YP, Chopra A, da Silva JAP, Kerstens PJSM, Lems WF, Tsonaka S, Huizinga TWJ, Allaart CF. Window or No Window? Earlier Is Better When Treating Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/window-or-no-window-earlier-is-better-when-treating-rheumatoid-arthritis/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/window-or-no-window-earlier-is-better-when-treating-rheumatoid-arthritis/