Session Information
Date: Sunday, October 26, 2025
Title: (0554–0592) Spondyloarthritis Including Psoriatic Arthritis – Treatment Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Psoriatic arthritis (PsA) is a chronic inflammatory disease combining psoriasis (Pso) and arthritis. Despite the availability of multiple therapeutic options, many patients experience residual disease activity and fail to achieve remission or low disease activity. Similar to rheumatoid arthritis, where the concept of “difficult-to-treat” (D2T) has emerged, studies are exploring its application to PsA.
Methods: A retrospective analysis of patients with PsA followed during at least two years treated with at least one bDMARD between 2010 and 2024 at Bellvitge University Hospital was conducted. Patients were stratified into two groups (D2T-PsA vs. “Good Responders” (GR)). D2T was defined as failure to ≥1 conventional synthetic DMARD (csDMARD) and ≥2 bDMARDs, and “GR” as those who failed to ≥1 csDMARD and <2 bDMARD that used during at least two years. Demographic, clinical, diagnostic, disease activity scores (including DAPSA, PASI) at baseline, 6 and 12 months, and therapeutic data were collected. Besides, bDMARDs number and reasons for their discontinuation were registered. Data were presented as frequencies and percentages for qualitative variables and as mean and standard deviation (SD) for quantitative variables. Chi-squared or Fisher's exact tests were used for the comparative analysis of qualitative variables, while the Student's t-test was applied to quantitative variables to identify differences between both groups.
Results: A total of 103 patients with PsA were included, of whom 40 (38.8%) were categorized as D2T. Clinical characteristics of both groups are shown in Table 1. While gender distribution was similar between groups (47.6 vs 51.5%), patients in the D2T group were significantly younger than the GR (p=0.022). Mean duration of Pso was around 28 years and PsA ranged 16-17 years in both groups. Cardiovascular risk factors did not differ between groups. Nonetheless, fibromyalgia (FM), as diagnosed by the rheumatologist, was more prevalent in the D2T group (p=0.006). No differences were observed in peripheral or extra-musculoskeletal manifestations, nail involvement, or serological features, including HLA-B27 positivity. Regarding disease activity, baseline DAPSA scores were similar between groups, while at 6 and 12 months post-bDMARD initiation, DAPSA scores were significantly higher in the D2T group than in GR (p=0.010 and 0.048, respectively). Baseline PASI scores were significantly higher in the D2T group at baseline (15.58 ± 8.45, p=0.017), although differences were not observed at 6 and 12 months. Tumour necrosis factor inhibitors were the most used bDMARDs in both groups. As seen in Figure 1, the most frequent reason for discontinuation was the primary inefficacy (52%) in the group of GR, while in the D2T group secondary inefficacy (40%) was the most frequent cause.
Conclusion: Around one third of PsA patients requiring bDMARDs met D2T criteria. This subset was characterised by younger patients with higher disease activity, greater severity of Pso, and a higher prevalence of FM, while we found no differences in baseline activity by DAPSA or other variables.
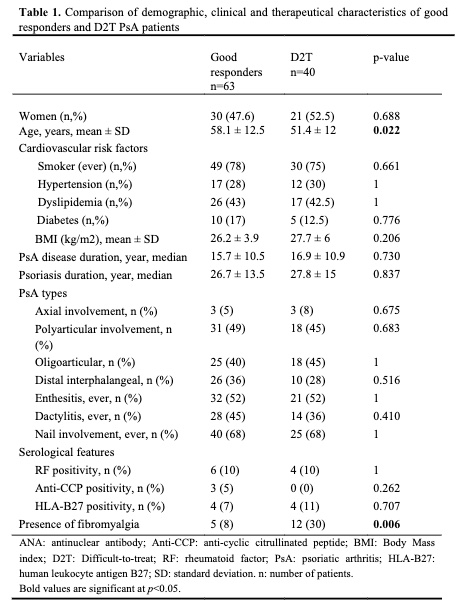 Table 1. Comparison of demographic, clinical and therapeutical characteristics of GR and D2T PsA patients
Table 1. Comparison of demographic, clinical and therapeutical characteristics of GR and D2T PsA patients
.jpg) Table 2. Comparison of disease activity characteristics of GR and D2T PsA patients
Table 2. Comparison of disease activity characteristics of GR and D2T PsA patients
.jpg) Figure 1: Comparison of the cause of discontinuation of the first bDMARD of good reponders and D2T
Figure 1: Comparison of the cause of discontinuation of the first bDMARD of good reponders and D2T
To cite this abstract in AMA style:
De Daniel Bisbe L, Rodriguez J, Berbel L, Nolla J, Fabregat A, Cubells M, Benavent Nuñez D. Why Do Some Psoriatic Arthritis Patients Fail Treatment? Exploring the Profile of D2T Patients [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/why-do-some-psoriatic-arthritis-patients-fail-treatment-exploring-the-profile-of-d2t-patients/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/why-do-some-psoriatic-arthritis-patients-fail-treatment-exploring-the-profile-of-d2t-patients/